research engineering @deepmind science | previously #graph#ML lead at @AstraZeneca, @biogen @targetvalidate | medicine @ImperialMed, engineering @mit_hst
How can you accelerate your day to day research workflow?
By giving AI the right scientific toolkit.
We launched Science Skills for Google @Antigravity, integrating insights from over 30 major life science sources, including UniProt and the AlphaFold Database.
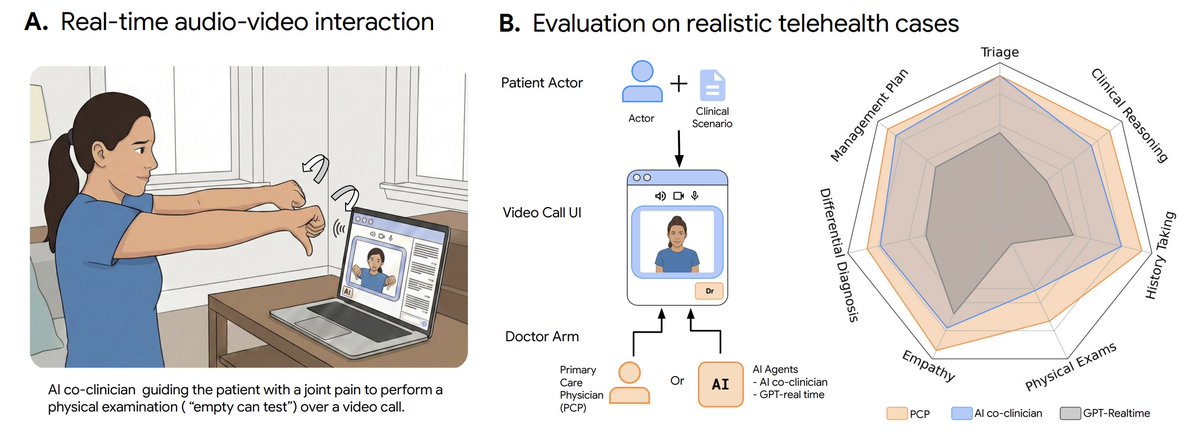
(1/10) Excited to share our new paper: "Towards Conversational Medical AI with Eyes, Ears and a Voice"
https://t.co/k0CNjqsgIP
Clinical medicine depends on more than words; it relies on real-time visual cues (rashes, distress, gait), auditory signals (prosody, breathing), and guided physical exams (e.g., guiding someone through correcting their inhaler technique, or walking them through shoulder maneuvers to work up a rotator cuff injury).
But existing conversational medical AI systems are blind and deaf to this crucial information and are constrained to rigid, turn-by-turn user experience.
As an important ingredient in AI co-clinician, our new healthcare initiative at @GoogleDeepMind, we developed a first-of-its-kind real-time multimodal system that conducts natural clinical consultations over video calls while continuously watching, listening, and reasoning.
The preprint details the research progress we’ve made so far together with our collaborators at @StanfordMed and @harvardmed (@AdamRodmanMD@euanashley@DrJackOSullivan@jasongusdorf).
More details below!
NEW: today OpenBind ‘comes out of stealth’ so to speak with their first data dump of ~900 novel protein-ligand structures - most with paired affinities
This represents a meaningful %-age increase in all of humanities P-L data in the PDB collected in the last 50 years
More👇
We’re advancing this research with academics and institutions globally, and will gradually expand our clinician-facing trusted tester program to additional sites - to understand more perspectives of health workers and patients worldwide.
Find out more → https://t.co/NanjCw7y9d
What biology can do with AI in the next few years depends on what gets measured, standardized, and shared today.
We're setting up our 4th(!) Impetus Grants @impetusgrants round to fund open, AI-enabling biological datasets, and we're currently assembling the review team.
If you want to learn more or contribute to this round, click here: https://t.co/5NJGQ78Gfk
We're launching the Anthropic STEM Fellows Program.
AI will accelerate progress in science and engineering. We're looking for experts across these fields to work alongside our research teams on specific projects over a few months.
Learn more and apply: https://t.co/MoF60j53pX
Introducing Claude Design by Anthropic Labs: make prototypes, slides, and one-pagers by talking to Claude.
Powered by Claude Opus 4.7, our most capable vision model. Available in research preview on the Pro, Max, Team, and Enterprise plans, rolling out throughout the day.
Every time I read a @CalebLareau tweetorial & paper, I feel very secure that there will always be some humans that will give AGI a run for it's money 😂😂😂. Super clever & innovative stuff.
📢 We’re launching Proteina-Complexa — and after the Jensen keynote mention, we definitely had to post this thread now ;)
Atomistic binder design with generative pretraining + test-time compute, plus large-scale wet-lab validation.
Project page: https://t.co/aT8Lz2VhSJ
🧵 1/n
claude code is dangerous for work life balance. i used to be good about not working at home. but 'type a few prompts and walk away' doesn't feel like working. until you realize you've been kicking off plan/implement cycles all evening trying to optimize your 4hr session limit.
Using Claude Code has a weird side effect: You don't just get more productive, you actually want to work more.
There's something addictive about watching a product being born in real time in front of your eyes.
"One last feature" after "one last feature" and it's already past 3am.
We simultaneously generated a single cell dataset from top gene knockouts, knockdowns, overexpressions, synthetic genes, and CAR signaling domains. The full set of potential phenotypes was only accessible by testing across perturbation classes, and the most divergent transcriptomic phenotypes correlated with the greatest CAR T cell functional enhancements.
We simultaneously generated a single cell dataset from top gene knockouts, knockdowns, overexpressions, synthetic genes, and CAR signaling domains. The full set of potential phenotypes was only accessible by testing across perturbation classes, and the most divergent transcriptomic phenotypes correlated with the greatest CAR T cell functional enhancements.
Recent advancements in one-shot AI protein / antibody development by Chai, Nabla, AI Proteins, Generate, and a few others are accelerating the *main* theme in biotech:
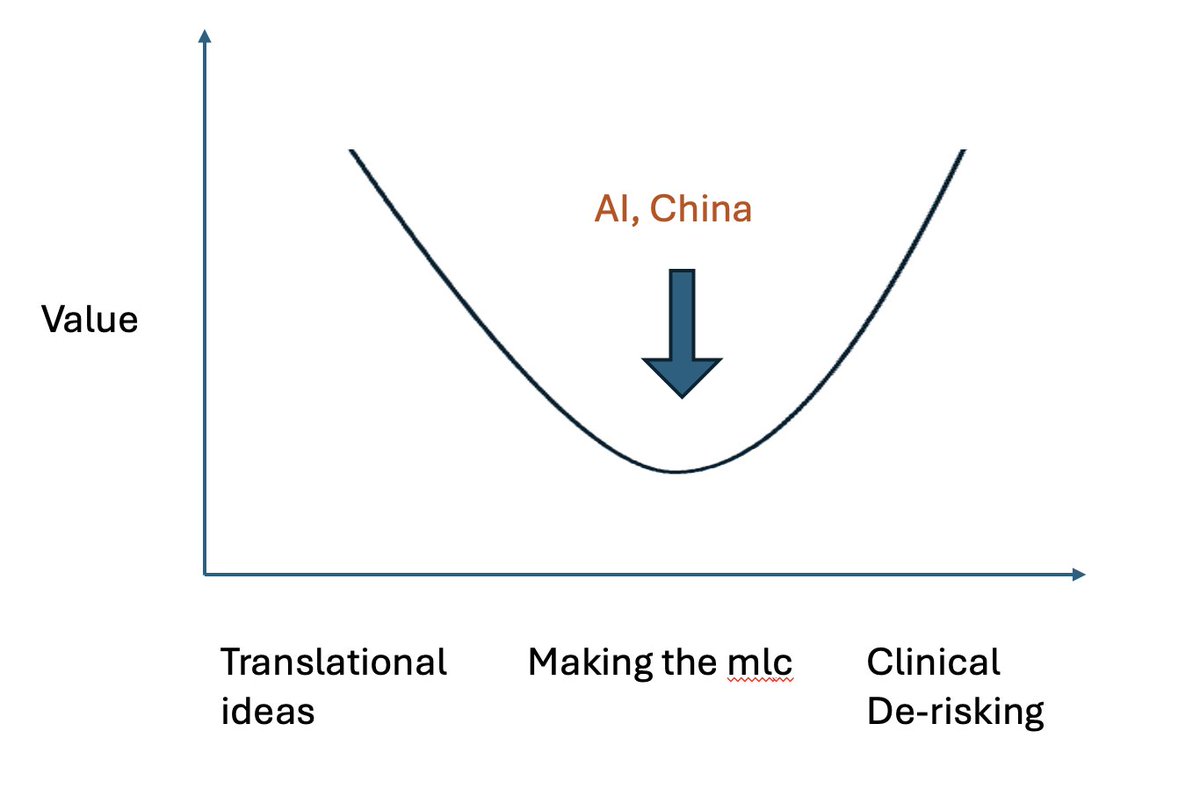
Value of building the molecule is going down. The value of novel targets, novel translational ideas, AND also the value of clinical execution is going UP
Here's where the value graph is moving towards:
The twin forces of AI and China are quickly driving down price of mlc dev across many modalities:
For AI - mainly Ab right now, emerging for genetic medicines, small mlc, ADCs, cell therapy;
For China - Abs, cell and gene therapy, small mlc, and soon genetic medicines
Having a "best in class" mlc is no longer enough - many tech platforms will soon offer you a mlc priced on metered compute (getting cheaper) and China CROs / biotechs will continue to eat the world with (over)capacity (continued involution).
To make a valuable drug, you must differentiate on either:
a) Novel translational ideas.
Novel targets, novel mechanisms, but not just that - connecting targets with diseases; novel application of certain targets in new disease settings, new intuition on which patient pops have widest therapeutic index for a drug, etc
OR
b) Clinical execution.
Determining the appropriate endpoints in a trial. Recruiting the right patients. Appropriate relationships with the right PIs / clinical sites. Ability to finance registrational studies in US markets ($10s to 100s of Ms)
Either be a translational target discovery engine / tech platform that unlocks new modalities (which unlocks new translational hypotheses) OR get a team of grizzled clin dev / CMO vets and go raise $X00M+ to validate a clinical hypothesis
Living in the middle (ie being "full stack") is dangerous work (at least for a startup)