Cochrane updated its PSA screening meta-analysis. 789,086 men across 6 RCTs.
➡️ PCa-specific mortality: rate ratio 0.87 (moderate certainty)
➡️ Metastatic diagnosis: RR 0.65
➡️ Adverse events / QoL: little to no difference
Why this matters: 💡 PSA screening is back on stronger evidentiary footing for disease-specific mortality. Shared decision making still drives the recommendation downstream and additional tools (biomarkers and MRI) continue to improve the gap.
https://t.co/VZk9tKRW0V
@EBMUrology #ProstateCA #Screening #Cochrane #GUonc #AUA26
Guideline of guidelines: lutetium-177 PSMA radioligand therapy in advanced prostate cancer
https://t.co/yb3G1t7bN2
Review synthesises international guidance on lutetium-177 PSMA radioligand therapy (177Lu-PSMA-RLT) in #ProstateCancer , focusing on metastatic castration-resistant disease. Major societies, including EAU, NCCN, ASCO, AUA/SUO, and CUA, endorse 177Lu-PSMA-617 after prior ARPI and taxane therapy, supported by VISION and TheraP trial data. Emerging evidence from PSMAfore is expanding use into earlier treatment settings.
Current recommendations emphasise PSMA-positive patient selection, standardised dosing, androgen deprivation therapy continuation, and multidisciplinary management.
@declangmurphy@DrMHofman@AzadOncology@RenuEapen@lawrentschuk@drMPerera@OncoAlert 🚨
@Silke_Gillessen@AOmlin@weoncologists
Back from an amazing @APCCC_Lugano!
Special thanks to @gu_onc for the GU Cast Travel Grant and their support of the next gen of Urology! Grateful for the opportunity
Inspired by new ideas, friends and connections
A pleasure meeting @UroTeragLATAM and fellow Chilean colleagues
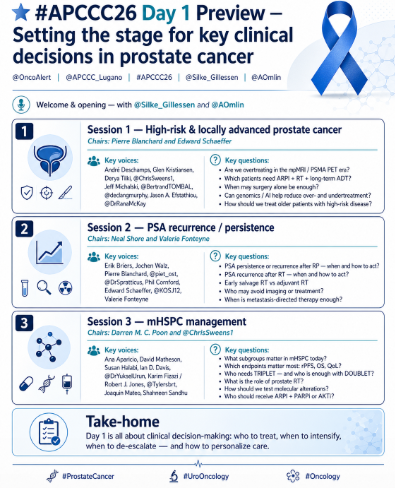
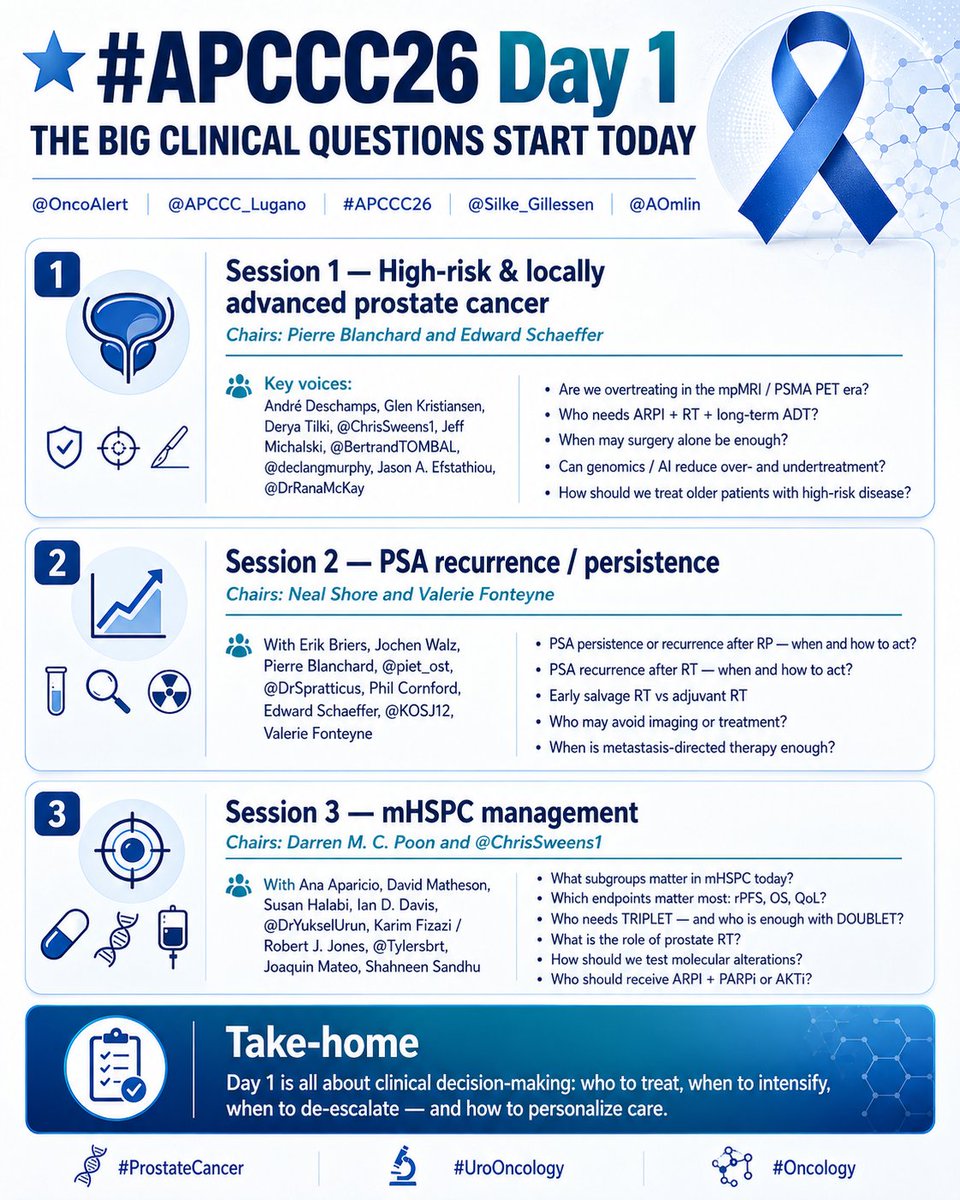
⭐ #APCCC26 Day 1 Preview — Setting the stage for key clinical decisions in prostate cancer
@OncoAlert@APCCC_Lugano#APCCC26@Silke_Gillessen@AOmlin
🔹 Welcome & opening
With @Silke_Gillessen and @AOmlin
🔹 Session 1 — High-risk & locally advanced prostate cancer
Chairs: Pierre Blanchard and Edward Schaeffer
Key voices today:
André Deschamps, Glen Kristiansen, Derya Tilki, @ChrisSweens1, Jeff Michalski, @BertrandTOMBAL, @declangmurphy, Jason A. Efstathiou and @DrRanaMcKay
🔹 Key questions:
• Are we overtreating in the mpMRI / PSMA PET era?
• Which patients need ARPI + RT + long-term ADT?
• When may surgery alone be enough?
• Can genomics / AI help reduce over- and undertreatment?
• How should we treat older patients with high-risk disease?
🔹 Session 2 — PSA recurrence / persistence
Chairs: Neal Shore and Valerie Fonteyne
With Erik Briers, Jochen Walz, Pierre Blanchard, @piet_ost, @DrSpratticus, Phil Cornford, Edward Schaeffer, @KOSJ12 and Valerie Fonteyne
🔹 Key questions:
• PSA persistence or recurrence after RP — when and how to act?
• PSA recurrence after RT — when and how to act?
• Early salvage RT vs adjuvant RT
• Who may avoid imaging or treatment?
• When is metastasis-directed therapy enough?
🔹 Session 3 — mHSPC management
Chairs: Darren M. C. Poon and @ChrisSweens1
With Ana Aparicio, David Matheson, Susan Halabi, Ian D. Davis, @DrYukselUrun, Karim Fizazi / Robert J. Jones, @Tylersbrt, Joaquin Mateo and Shahneen Sandhu
🔹 Key questions:
• What subgroups matter in mHSPC today?
• Which endpoints matter most: rPFS, OS, QoL?
• Who needs TRIPLET — and who is enough with DOUBLET?
• What is the role of prostate RT?
• How should we test molecular alterations?
• Who should receive ARPI + PARPi or AKTi?
🔹 Take-home:
Day 1 is all about clinical decision-making:
who to treat, when to intensify, when to de-escalate — and how to personalize care.
@declangmurphy@RenuEapen@DrYukselUrun@fabioturco92@UrsulaVogl @SScagliarini @Tylersbrt@neerajaiims@amerseburger@Cdanicas@AarmstrongDuke@BertrandTOMBAL@ChrisSweens1@EAntonarakis@KOSJ12@VedangMurthy@DrRanaMcKay@LoebStacy@stefanofanti4@mirrorsmed @profkhermann @dr_coops@piet_ost@_ShankarSiva@DrSpratticus@scocmem@AmandaNizamMD@tompowles1@brian_rini@Uromigos@EUplatinum@EANM_NucMed@ESTRO_RT@Uroweb
#ProstateCancer #UroOncology #Oncology
It's Testicular Cancer Awareness Month! Do you know how your pair is hanging?
Testicular cancer is the #1 cancer among young guys but it's highly curable when caught early.
If you’ve got ’em, check your nuts.
Head to https://t.co/J99jtSDNYk to learn how.
⚡️ NICE 2026 kidney cancer guideline (diagnosis & management) — updated pathway from suspicion → staging/biopsy → risk-adapted treatment & follow-up.
Striking stat: 87% of UK stage 1a RCC is diagnosed incidentally, underscoring how hard early detection is in routine practice.
#KidneyCancer @OncoAlert
https://t.co/O6xWOoleIv
Proud moment and HUGE news from #EAU26: #PRIMARY2 shows PSMA PET/CT can safely halve prostate biopsies in men with equivocal MRI, avoiding biopsy in 49% without missing cancer. https://t.co/OOGooac59C
ICYMI, the GU Cast Live Show at #EAU26 in London now streaming on all our channels. What a fantastic evening with so many of our listeners/viewers. Thanks so much to @MaartenAlbersen@Uroweb for the invite. Enjoy the replay! @declangmurphy@RenuEapen https://t.co/AWqF3Gxvzw
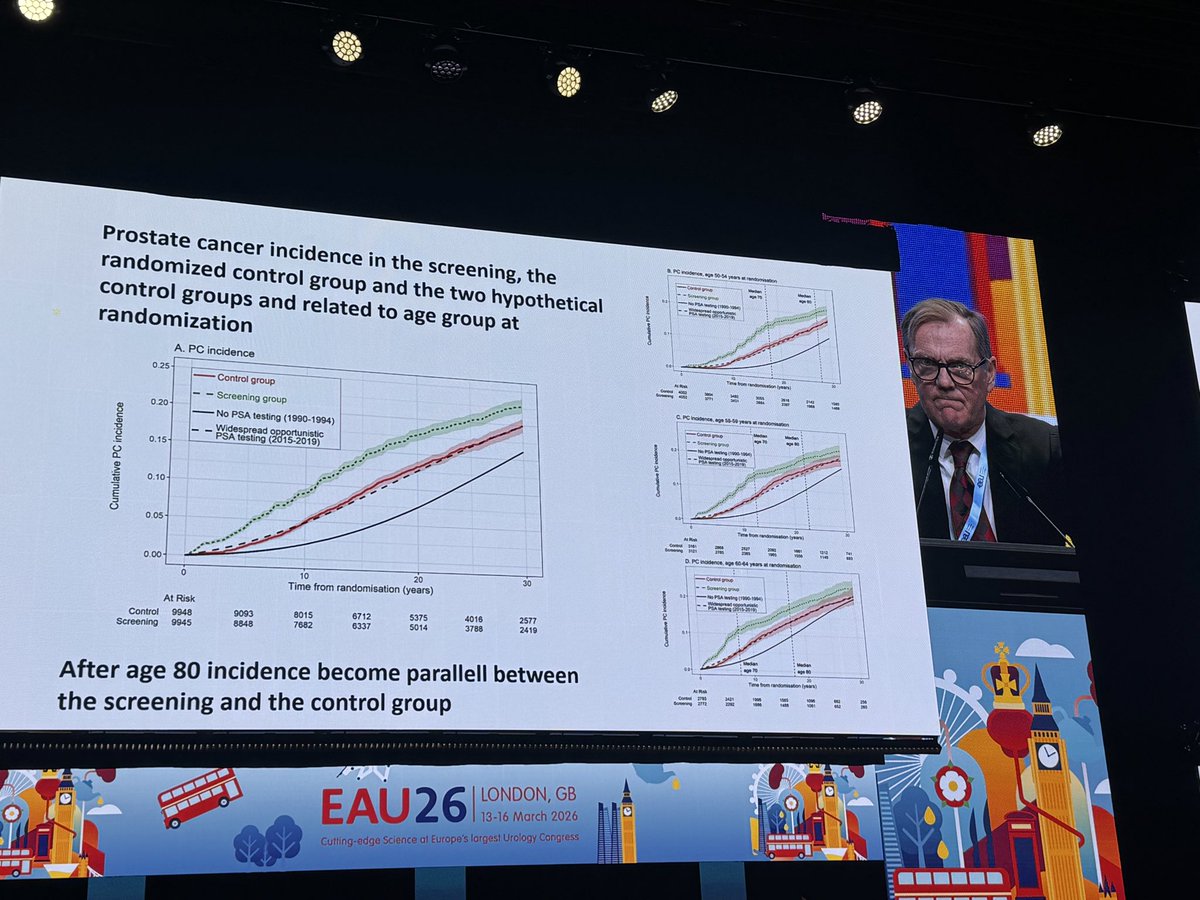
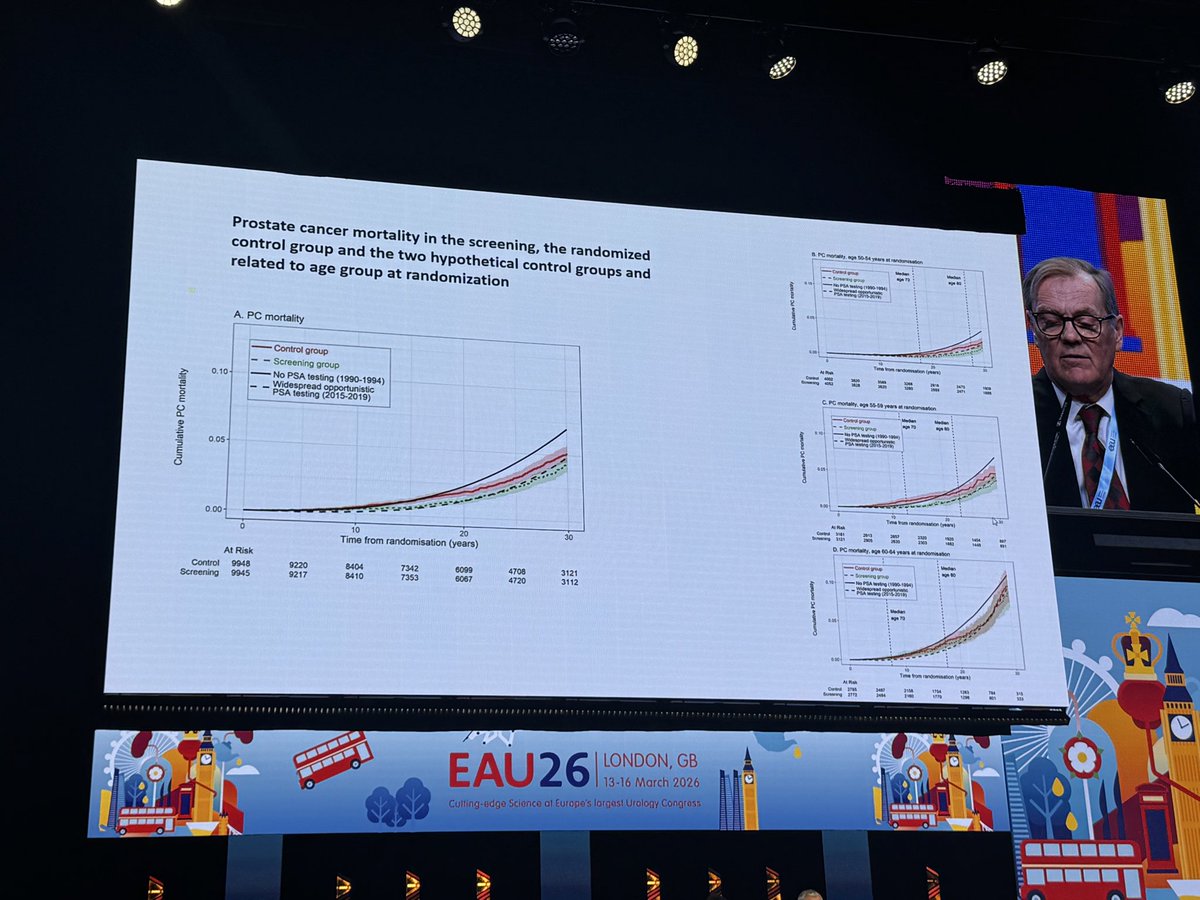
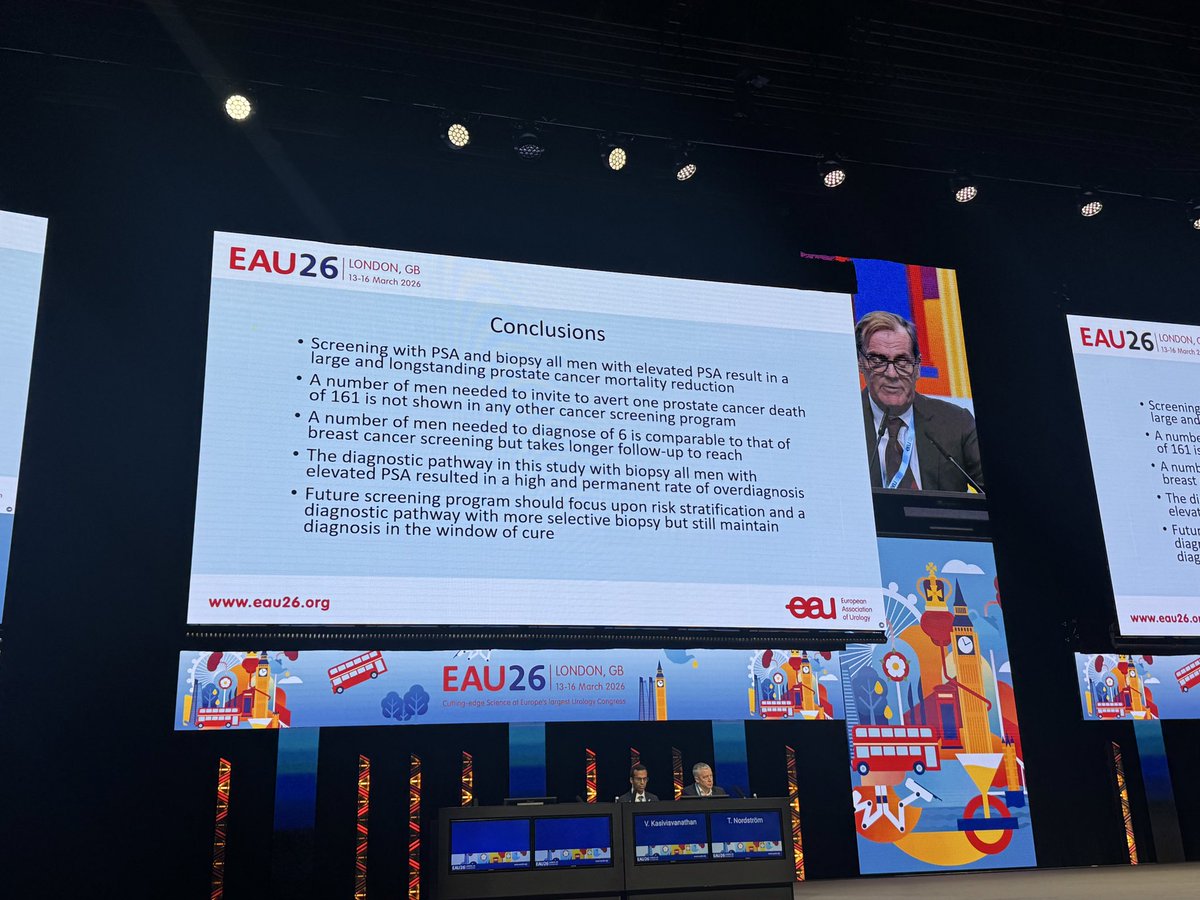
Prof Hugosson: Göteborg trial with 30 year outcomes! NND falls to -6-, with greatest benefit for men 50-59 at randomization. Despite no image guidance, high overdx, and suboptimal tx. Best evidence we have re: the evidence for #prostatecancer screening. Get tested! #eau26@uroweb
In October 2025 we presented our study on the impact of Public Health Policy for Testicular Cancer in Chile at Congreso @Urolchi 2026, demonstrating improved Overall Survival after implementation.
We won best Oral presentation and today en route to #EAU26 thanks to this prize 🏆
It’s disappointing to me that TURBT continues to be dismissed as a “low-priority” procedure in so many training programs.
This single step defines the entire course for a bladder cancer patient. Accurate diagnosis, precise staging, and the choice of therapy all hinge on a high quality TURBT.
And the “advanced genomic analysis and molecular profiling” these same programs love to promote? It all begins with adequate, high-quality tissue obtained through a TURBT.
Yet incomplete resections leave behind residual tumor in up to 78% of cases at restaging, leading to higher recurrence rates and unnecessary progression.
If we are serious about improving outcomes in NMIBC - and even MIBC - we must treat TURBT with the respect it deserves: structured, deliberate training curricula, hands-on attending involvement, and real performance metrics.
This is why the @IBCG_BladderCA will make this one of the focus topics of our retreat this year, #IBCG26
@UrogerliMD@JoshMeeks@bbmdmsk@siadaneshmand@RobertoContieri@paolo_gontero@ParamMariappan@joanfundi@jteoh_hk@spsutkaMD@WorldBladderCan@BladderCancerUS@drgaganprakash@SUO_YUO@veerukasi
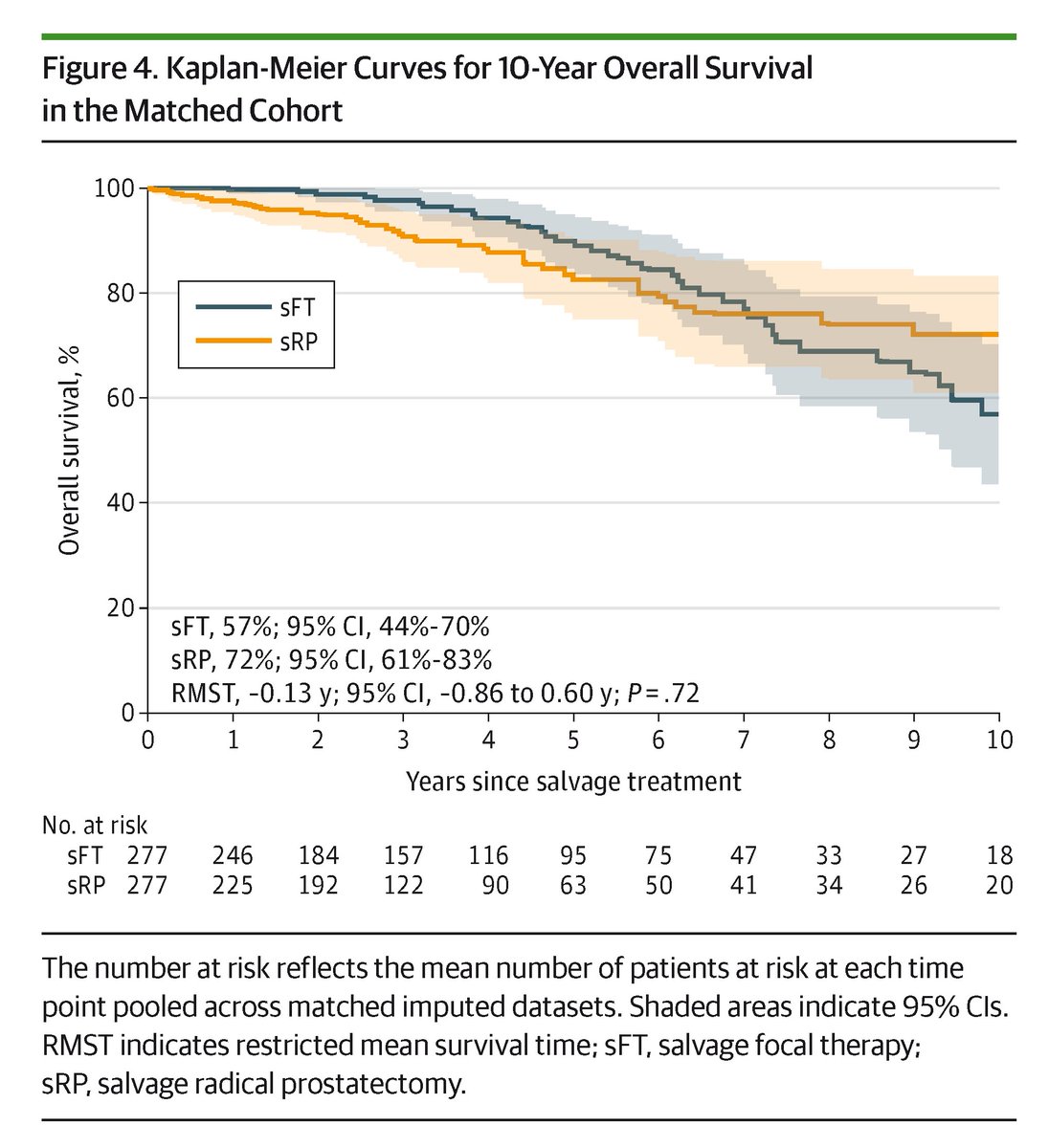
In localized radiorecurrent #ProstateCancer, salvage focal therapy provided similar 10-year survival outcomes as radical prostatectomy but resulted in substantially fewer perioperative complications.
https://t.co/jTGubKb4Zn
📰 Is audit enough to improve TURBT quality? Insights from the RESECT trial reveal improved outcomes, but can it be implemented in clinical routine? Commentary by Dr. Elisabeth Grobet-Jeandin (@elijeandin). #NMIBC#bladdercancer 👇
https://t.co/z0LMwCi4xf
📅 Les compartimos el calendario anual de SCHU, que incluye nuestras actividades académicas oficiales, además de las iniciativas patrocinadas y las internacionales.
Esperamos que puedan organizar y planificar sus agendas para que puedan participar en estas actividades.