Extremely proud to announce that our NEOPREDICT-Lung study on neoadjuvant PD-1 and LAG-3 inhibition in resectable NSCLC is now online in @NatureMedicine . Without any doubt one the highlights of my career so far.
https://t.co/DHuktFCTtQ
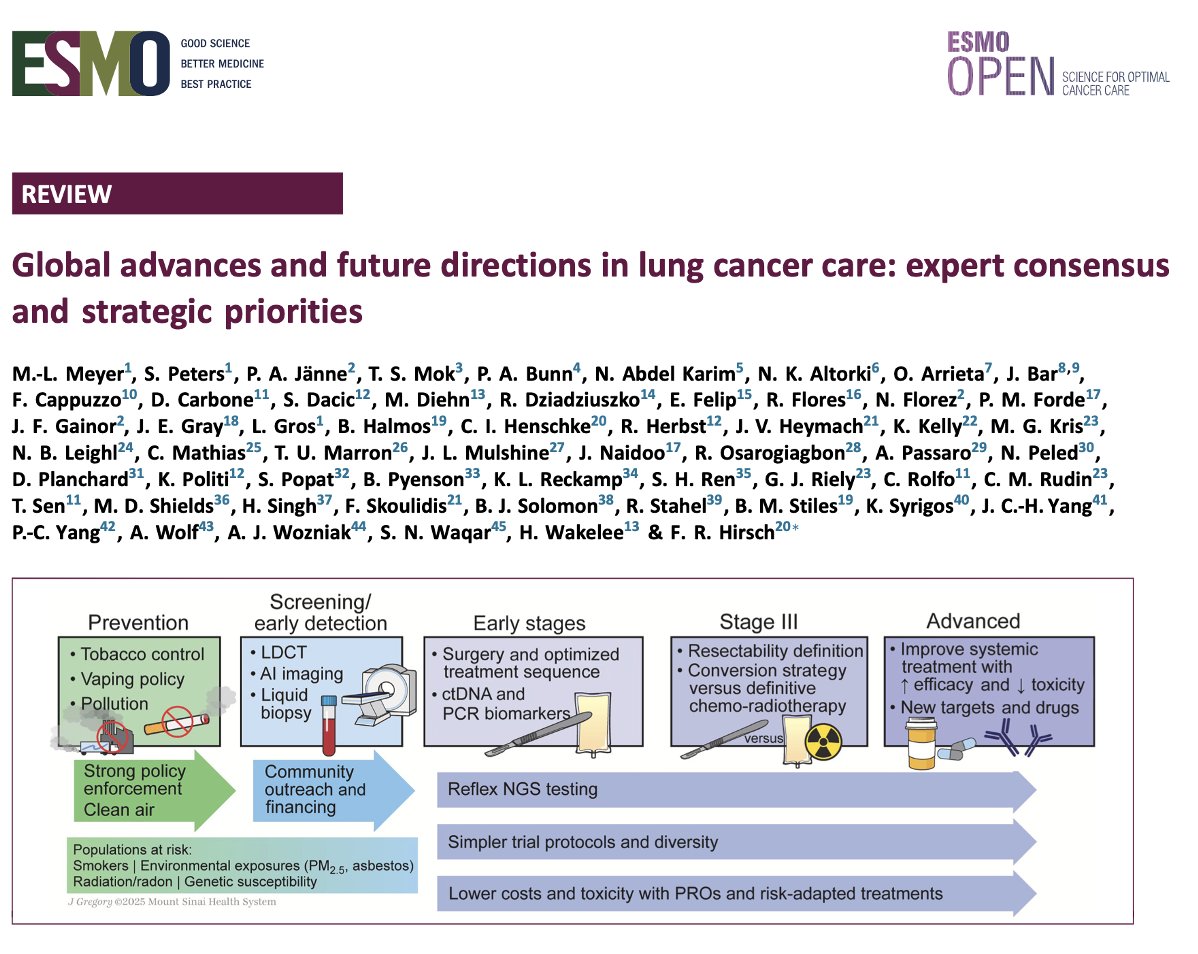
Global advances and future directions in lung cancer care: expert consensus and strategic priorities in @ESMO_Open. Important advances but global disparities, limited trial access, & implementation challenges still hinder progress. https://t.co/P3XbXn6e80
Update on CheckMate 77T (addition of perioperative nivolumab to neoadjuvant chemo in resectable NSCLC) @NatureCancer. In stage III N2+ NSCLC: EFS HR 0.46, 1y EFS 70% vs 45%, pCR 22% vs 5.6% - in multistation N2, EFS 0.43! Profound benefit here.
https://t.co/2JxQUQLyDK
@DrJNaidoo@NatureComms@gecp_org@MARIANOPROVENCI Besides the very promising outcome of APOLO , this imo also provides more confidence for chemo-IO upfrontMDT-Bridge strategy in “borderline resectable” stage III NSCLC
results of the phase I/II study of therapeutic cancer vaccine PDC∗lung01 with or without anti-PD-1 in NSCLC is now published in ESMO open @myESMO@JessaZiekenhuis@GLW_UHasselt@JessaWetenschap https://t.co/8uFPyTobNd
🫁 #ASCO2025 In-Depth! Dr @k_cupp_ on SACHI :
✔️ Oral savolitinib + osi
✔️ PFS: 7–8 vs 4 mo vs chemo
✔️ Good tolerability
👀 Watch now https://t.co/v4Gf0RbGFN #MediMix#NSCLC#EGFR#MET
🫁 #ASCO2025 In-Depth! Dr @k_cupp_ on SACHI :
✔️ Oral savolitinib + osi
✔️ PFS: 7–8 vs 4 mo vs chemo
✔️ Good tolerability
👀 Watch now https://t.co/v4Gf0RbGFN #MediMix#NSCLC#EGFR#MET
And let’s not forget the proportion of patients that don’t even get to therapy due to inadequate testing for AGAs or have no access to appropriate treatments
Real-world data on 1323 EGFR+ NSCLC pts on 1L osimertinib:
• Median OS: 28.6 mo
• High-risk pts:
- TP53: 25.7
- Brain mets: 24.3
- Liver mets: 19.3
- ECOG ≥2: 18.1
This isn’t good enough. Patients & families deserve more.
https://t.co/JpYjRhKkn8
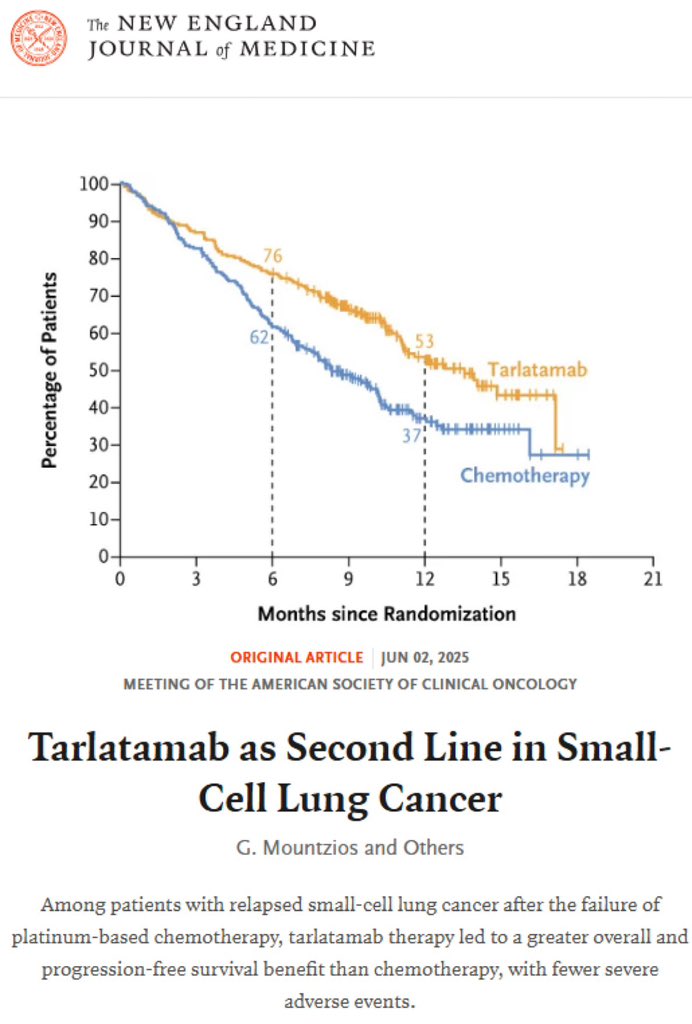
#ASCO25 After 30 years of failed trials, #tarlatamab changes SoC for our pts with relapsed #SCLC :
✅ mOS: 13.6 vs 8.3 months, HR=0.6, p<0.001
✅ improved QoL (dyspnea and cough)
✅ 27% vs 62% G3 TRAEs
Grateful to all collaborators, @Amgen science team and above all our pts
#ASCO25 Dr. @charlesrudin presents interim analysis of DeLLphi-304: randomized phase II study of tarlatamab (DLL3 TCE) vs 2L chemo in #SCLC. Chemo was mostly topotecan; 45% of pts were platinum resistant. Clear OS benefit with HR 0.60 (13.6m vs 8.3m). PFS 4.2 vs 3.7m, HR 0.71.
Another breakthrough for our SCLC patients! Based on personal experience, this regimen is well tolerated when properly managed. Proud that our site @JessaZiekenhuis has yet again significantly contributed to a practice changing study.
@JessaWetenschap@GLW_UHasselt
IMforte: RP3 maintenance lurbi+atezo ES-SCLC
CNS+ excluded. Enrolled post #4 chemo-atezo if non-PD. GCSF supported.
PFS HR=0.5: 2.1 to 5.5mo
OS HR=0.73: 10.6 to 13.2mo (from randomztn)
ORR 19.4 vs 10.4mo
AEs as expected
Bravo: a new standard of care #ASCO25
IMforte: RP3 maintenance lurbi+atezo ES-SCLC
CNS+ excluded. Enrolled post #4 chemo-atezo if non-PD. GCSF supported.
PFS HR=0.5: 2.1 to 5.5mo
OS HR=0.73: 10.6 to 13.2mo (from randomztn)
ORR 19.4 vs 10.4mo
AEs as expected
Bravo: a new standard of care #ASCO25
Results of Delphi-304 usher a new era for SCLC patients. Finally a truly game changer in the fight against this frightening disease. Immensely proud to have been part of this study. @ASCO@JessaZiekenhuis@JessaWetenschap@GLW_UHasselt@g_mountzios
https://t.co/nrFIN1XeNt
Being part of a history-making drug that helps pts with #SCLC live longer and better is the biggest reward a thoracic oncologist could hope for.
Grateful being involved and to our pts
Just out in @NEJM
Presentation today by 1@only @charlesrudin#ASCO25