Supplementation with Vitamin D or calcium, or both does not help prevent fractures or falls. From a new systematic review of 69 randomized trials and >150,000 participants
🩺 Obesity-related hypertension — it’s not just about weight.
In 77 patients with obesity-related HTN, dynamic hormonal phenotyping (saline suppression, ACTH stimulation, dexamethasone testing) revealed:
🔴 51.9% — Primary aldosteronism phenotype
🔵 23.4% — Renin-dependent aldosteronism
🟡 24.7% — Low-renin phenotype
⚪ 9.2% — ACTH-independent hypercortisolism
The striking finding? Over 80% had overlapping pathologic phenotypes of aldosteronism and/or hypercortisolism.
➡️ Obesity-related hypertension is far more hormonally complex than we think — and static phenotyping alone misses a large part of the picture.
Could targeted hormonal workup change how we treat these patients? 🧵
Parisien-La Salle S. et al. — JACC Basic Transl Sci. 2026;11(4):101526
#Hypertension #Obesity #Aldosteronism #Endocrinology #Cardiology #MedTwitter #CardioTwitter #JACC #Hypercortisolism #Hormones
Switching from OHAs ± Insulin to GLP-1 RA: A Metabolic Re-Engineering Approach
Transitioning from oral hypoglycemic agents (OHAs) with or without insulin—whether premixed human insulin (70% NPH + 30% Regular) or basal insulin such as —to a GLP-1 receptor agonist is not a drug substitution.
It represents a strategic metabolic shift targeting weight reduction, glycemic stability, and cardiovascular risk modification.
CME INDIA – Practical Stepwise Guide
1. Identify the Right Candidate
GLP-1 RA therapy is best suited for:
Overweight or obese T2D (BMI ≥27 kg/m²; high visceral adiposity in Asian Indians)
Suboptimal control on OHAs ± insulin
Established ASCVD or high cardiovascular risk
Need to reduce insulin dose or minimize hypoglycemia
NAFLD / metabolic syndrome phenotype
Use caution in:
Prior pancreatitis
Severe gastroparesis
Medullary thyroid carcinoma / MEN2
2. Baseline Clinical Assessment (Non-negotiable)
Before initiating the switch:
HbA1c (defines transition intensity)
Renal function
Weight and waist circumference
Hypoglycemia history
Current insulin pattern (premix vs basal)
Retinopathy status in long-standing diabetes
3. Strategy Based on Existing Therapy
A. Patient on OHAs Alone
Continue metformin
Discontinue sulfonylurea (reduces hypoglycemia risk)
Discontinue DPP-4 inhibitor (mechanistically redundant)
Initiate GLP-1 RA at low dose and titrate gradually
B. Patient on Premixed Insulin (70% NPH + 30% Regular)
This is the most critical transition scenario.
Preferred approach:
Deconstruct premix regimen
Convert to basal insulin (~60–70% of total daily premix dose)
Initiate GLP-1 RA concurrently
Alternative cautious approach:
Continue premix initially but reduce dose by 30–50%
Add GLP-1 RA
Transition to basal-only regimen over 1–2 weeks
Clinical rationale:
Premixed insulin contains a fixed prandial component, increasing hypoglycemia risk when combined with GLP-1 RA, which already provides postprandial glucose control.
C. Patient on Basal Insulin
Continue basal insulin
Reduce dose by 20–30% at initiation
Add GLP-1 RA
Down-titrate insulin based on fasting glucose trends
4. Initiation of GLP-1 RA
Common agents include:
(weekly)
(daily)
(weekly)
Principles:
Start low, titrate slowly
Escalate every 2–4 weeks
Counsel regarding transient gastrointestinal effects
5. Glycemic Transition Logic
HbA1c >9% → Avoid abrupt insulin withdrawal
HbA1c 7–9% → Gradual insulin de-escalation
HbA1c <7% → Early insulin discontinuation may be feasible
6. Monitoring During Transition
The first 2–4 weeks are decisive:
SMBG or CGM monitoring is essential
Watch for:
Hypoglycemia (if insulin/SU not reduced appropriately)
Gastrointestinal intolerance
Rapid glycemic fall (retinopathy risk in vulnerable patients)
7. Expected Clinical Gains
HbA1c reduction ~1–1.5%
Clinically meaningful weight loss (3–8 kg, agent dependent)
Reduction or elimination of insulin requirement
Cardiovascular and renal protection (agent-specific evidence)
CME INDIA Clinical Pearls
“Never combine DPP-4 inhibitor with GLP-1 RA—mechanistically redundant.”
“Premixed insulin must be dismantled before GLP-1 RA integration.”
“GLP-1 RA replaces prandial physiology, not basal insulin.”
“Reduce insulin proactively to prevent reactive hypoglycemia.”
“Retinopathy worsening is driven by rapid glucose fall—not the molecule.”
“In obese Indian phenotype, introduce GLP-1 RA early—not as a rescue therapy.”
Tagline
“Switching to GLP-1 RA is not escalation—it is metabolic correction.”
@cmeindia1
New ACC/AHA Lipid Guidelines 2026 — Practice-Changing Insights:At a glance..
📌 Core Philosophy
“Lower LDL-C, earlier and for longer → better lifetime ASCVD reduction.”
🔬 1. Start Early – Think Lifetime Risk
Lipid screening should begin at ≥19 years, with repeat every 5 years or earlier in high-risk individuals.
Statin therapy can be initiated as early as 30 years if LDL-C ≥160 mg/dL, strong family history, or high 30-year risk—even if 10-year risk is low.
🎙️Key shift: Move from “10-year risk” to lifetime cumulative exposure model
🧮 2. PREVENT Risk Calculator Replaces PCE
New AHA PREVENT tool improves ASCVD risk prediction and starts risk estimation from age 30.
Includes 30-year risk estimation, crucial for younger patients.
📊 3. Recalibrated Risk Categories
Low: <3%
Borderline: 3–5%
Intermediate: 5–10%
High: ≥10%
👉 Clinical implication: Statins now justified at lower thresholds (≥5%)
🎯 4. LDL-C Targets Are Back
<100 mg/dL → Low/intermediate risk
<70 mg/dL → High risk
<55 mg/dL → Established ASCVD
👉 Shift: From % reduction → absolute target-driven therapy
🧬 5. Universal Lp(a) Testing
One-time Lp(a) measurement for ALL patients is now recommended.
≥125 nmol/L → ↑ ASCVD risk
≥250 nmol/L → ~2× risk
≥430 nmol/L → ~4× risk
👉 Intensify LDL lowering even if Lp(a) cannot yet be directly treated
🧪 6. ApoB & CAC — Precision Risk Tools
ApoB reflects total atherogenic particle burden and helps detect residual risk.
CAC score acts as “tiebreaker” in borderline/intermediate risk.
⚠️ 7. Expanded Risk Enhancers
Now includes:
PCOS, early menopause, adverse pregnancy outcomes
South Asian and Filipino ethnicity
CKM syndrome, inflammation markers
👉 Clinical message: Take detailed reproductive & ethnic history seriously
🩺 8. Special Populations – Stronger Statin Mandate
All patients (40–75 yrs) with:
CKD stage 3–4
HIV infection
→ Should receive statins irrespective of LDL-C
🍔 9. Triglycerides – Lifestyle First
Statins remain foundational even in hypertriglyceridemia.
Refer to dietitians if TG ≥150–1000 mg/dL with CKM features.
💊 10. Supplements – Clear Negative Recommendation
Non-prescription supplements (e.g., fish oil) are NOT recommended for ASCVD risk reduction due to lack of benefit.
🔥 CME INDIA Take-Home Messages
Atherosclerosis begins early → intervene early
LDL exposure = cumulative toxin → duration matters as much as level
Lp(a) is now a universal risk marker, not optional
Risk assessment is shifting from short-term to lifetime biology
Precision lipidology = LDL-C + ApoB + Lp(a) + CAC
🏷️
“From numbers to lifetime exposure: Lipidology has entered the era of precision prevention.”
https://t.co/HU2Fcucaf3
भेडा त आखिर भेडा नै हुन्, तर अचम्म त के भने मान्छे पनि भेडा नै हुँदा रहेछन्। फरक यति हो— सक्कली भेडालाई गोठालोले धपाउँछ, नक्कली भेडा (मान्छे) चाहिँ आफैं खाल्डोतिर दगुर्छन्!
@sudeepkhaniya नेपाल को स्टोरी अर्कै छ | Obesity को Guideline nepal मा छैन तेसैले नेपाल मा येस्को आवस्यक नहुन पनि सक्छ रे | हामि Primitive medicine र जडिबुटि मै Focus गरेको राम्रो | तेता Guideline चाहिदैन |
Prenatal exposure to acid-suppressive medication, including proton pump inhibitors and histamine 2 receptor antagonists, was not associated with increased risk of #ADHD, #ASD, or other neuropsychiatric disorders in children.
https://t.co/kLx5xJwZaG
⚖️💊 What happens when weight-loss drugs stop? The uncomfortable truth
This 2026 BMJ systematic review and meta-analysis delivers one of the clearest reality checks yet on weight regain after stopping weight-management medications (WMMs), including GLP-1 and dual incretin therapies .
🔍 What was studied
Across 37 studies (63 treatment arms, 9,341 adults) with overweight or obesity, the authors quantified how fast weight returns after discontinuing medication, and compared this with regain after behavioural weight-management programmes (BWMPs). Follow-up extended up to two years after treatment cessation.
📉 The headline finding
On average, people regain 0.4 kg per month after stopping WMMs. At this pace, baseline weight is reached again within ~1.7 years.
For newer, highly effective incretin drugs (e.g. semaglutide, tirzepatide), regain is even faster—up to 0.8 kg/month, with return to baseline in ~1.5 years.
🫀 Metabolic benefits fade too
Improvements in HbA1c, fasting glucose, lipids, and blood pressure closely track weight. Once medication stops, cardiometabolic markers steadily worsen, returning to baseline within ~1.4 years. Weight loss without maintenance = temporary risk reduction.
⚠️ Worse than lifestyle alone
When directly compared, weight regain after stopping drugs was significantly faster than after stopping behavioural programmes, independent of how much weight was initially lost. Bigger losses tended to rebound faster—biology pushes back hard.
🧠 Why this matters
Obesity behaves like a chronic, relapsing disease. Short-term pharmacotherapy without a long-term plan risks disappointment, lost benefit, and misaligned expectations—for patients and health systems alike.
🔮 Bottom line
Weight-loss drugs are powerful—but they don’t “cure” obesity. Their benefits persist only while treatment continues, or if embedded in a sustained, comprehensive strategy.
Stopping therapy doesn’t just pause progress—it reverses it 🚨
Type 2 diabetes is no longer viewed as an inevitably progressive disease. Remission is now an evidence-based goal: bariatric surgery, pharmacotherapy (SGLT2i, GLP-1 RAs), and intensive lifestyle programs can all normalize A1c. The challenge for clinicians is less “can we induce remission?” and more “how do we scale and sustain these interventions in real-world practice while keeping lifestyle at the center and meds as the adjunct?” @TheAACE
https://t.co/ZHFYuGYmys
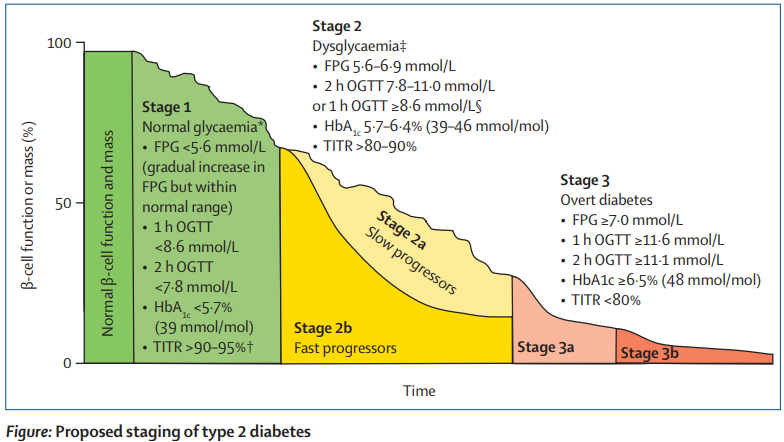
NEW: "Staging prediabetes and type 2 diabetes: the time to start is now"
Viral N Shah and colleagues propose a model for type 2 diabetes that assumes gradual decline in β-cell function or mass over time in people at risk for developing type 2 diabetes.
https://t.co/hKTVw4n3kE
ADA Standards of Care 2026: The New Algorithm for Glucose-Lowering Therapy in Type 2 Diabetes
The ADA 2026 reinforces a priorities-first approach:
1️⃣ Reduce cardiovascular & kidney (CVKD) risk
2️⃣ Manage weight
3️⃣ Achieve glycemic goals
4️⃣ Address MASLD/MASH risk
All built on a foundation of healthy lifestyle + DSMES + addressing SDOH.
🔶 1. FIRST PRIORITY: Cardiovascular & Kidney Risk Reduction
A. ASCVD or Indicators of High CV Risk
Preferred: GLP-1 RA with proven CV benefit
Alternative / Add-on: SGLT2i with proven CV benefit
If HbA1c above target → combine GLP-1 RA + SGLT2i
B. Heart Failure (HFpEF or HFrEF)
Preferred: SGLT2 inhibitor
Add GLP-1 RA (proven benefit) if glycemia not controlled or if comorbid obesity
C. CKD (eGFR <60 OR ACR ≥30 mg/g)
Preferred: SGLT2i with primary evidence of CKD protection
If eGFR <45 → GLP-1 RA with proven renal benefit
If glycemia above goal → combine SGLT2i + GLP-1 RA
If more CVKD risk reduction is needed
➡️ Add agents with proven benefit, treat lipids/BP aggressively, and reassess every 3–6 months.
🔶 2. SECOND PRIORITY: Weight Management
ADA 2026 clearly states:
Weight reduction itself is a therapeutic target in T2DM.
Weight-loss efficacy of medications (ADA 2026)
Very High: Semaglutide, Tirzepatide
High: Dulaglutide (high dose), Liraglutide
Intermediate: GLP-1 RA (others), SGLT2i
Neutral: DPP-4 inhibitors
Use GLP-1 RA / dual GIP-GLP-1 RA early in patients with obesity or weight-related complications.
🔶 3. THIRD PRIORITY: Glycemic Control
Efficacy for glucose lowering (ADA 2026)
Very High: Semaglutide, Tirzepatide, insulin combination therapy
High: GLP-1 RA, SGLT2i, Metformin, TZD, Sulfonylureas
Intermediate: DPP-4 inhibitors
If HbA1c remains above target → Stepwise intensification without delay.
🔶 4. NEW FOCUS 2026: MASLD/MASH (Metabolic Liver Disease)
ADA now adds a dedicated pathway:
Drugs with proven / potential benefit
GLP-1 RA
Dual GIP–GLP-1 RA
Pioglitazone
GLP-1 RA + Pioglitazone combination
⚠️ Use insulin in decompensated cirrhosis only.
🔶 5. When Treatment Goals Are Not Reached
Reassess every 3–6 months
Evaluate:
Barriers to care
Hypoglycemia risk
Adherence
Affordability
SDOH (social determinants of health)
⭐ CME INDIA Take-Home Messages
1️⃣ ADA 2026 is no longer “HbA1c-first”—it is “Heart–Kidney–Weight–Glycemia” in that order.
2️⃣ GLP-1 RA & SGLT2i dominate all therapeutic pathways due to CVKD & weight benefits.
3️⃣ Obesity is treated as a biological disease—not a lifestyle failure.
4️⃣ MASLD/MASH enters mainstream diabetes management for the first time.
5️⃣ Reassessment every 3–6 months is mandatory—clinical inertia is unacceptable.
https://t.co/wRp6gaKDvK
Today is One Health Day.
The health of humans, animals and ecosystems are closely interlinked. Changes in these relationships can increase the risk of new human and animal diseases developing and
spreading.
#OneHealth is an approach to optimize the health of humans, animals and ecosystems by integrating these fields, rather than keeping them separate https://t.co/hqaOeeiBvV
Future Glucose-Lowering Therapies (Beyond Insulin)
Diabetologia 2025
@medflutter_@drsthanus @DrAkhilX
@Medicalgur@official_aimsa@DiabetologiaJnl@AskDrShashank@DrKhushboo_Endo
🔹 1. Expanding Horizons in T2DM Pharmacotherapy
Diabetes management is evolving from glucose-centric to pathophysiology-centric approaches targeting beta cells, liver, kidney, gut, brain, and adipose tissue.
New drugs are focusing on restoring metabolic flexibility, preserving beta-cell function, and reducing organ-specific insulin resistance.
🔹 2. Six Core Therapeutic Targets
Beta Cells – Insulin Releasers/Activators
Imeglimin, Glucokinase activators, Fatty acid receptor agonists → enhance first-phase insulin release and beta-cell preservation.
Liver – Gluconeogenic Inhibitors
Direct metabolic modulators (AMPK activators, sirtuins, miRNAs) → reduce hepatic glucose output and lipogenesis.
Muscle – Insulin Action Enhancers
AMPK activators, FGF21 analogues → improve glucose uptake and mitochondrial efficiency.
Adipose Tissue – Metabolic Regulators
PPAR modulators, DGAT1 inhibitors → rebalance energy metabolism and counter insulin resistance.
Kidney – Glucosuric Agents
SGLT2/SGLT1 inhibitors → dual blockade enhances glucose elimination safely, even in CKD.
Gut–Brain Axis – Incretin/Amylin Pathway
GLP-1, GIP antagonists, Amylin analogues, Microbiome modulators → dual benefits on appetite and metabolic homeostasis.
🔹 3. Novel Agent Spotlight: Imeglimin
🧬 Mechanism
A tetrahydrotriazine compound acting on mitochondria to:
Boost NAD production via NAMPT.
Enhance ATP generation by stimulating respiratory complexes I & III.
Reduce oxidative stress and beta-cell apoptosis.
🧩 Key Clinical Effects
Improves glucose-induced insulin secretion (notably first-phase response).
Preserves beta-cell mass and function in early diabetes.
Reduces lipotoxicity and inflammation, enhancing insulin sensitivity.
🌍 Regulatory Milestones
Approved in Japan (2021) and India (2022).
Represents the first in its class “Mitochondrial Bioenergetic Modulator” for T2DM.
🔹 4. Microbiome & Gut-Based Therapies
SGLT1 inhibitors and microbiome modulators (pre-/probiotics) aim to delay glucose absorption and remodel incretin pathways.
Potential synergy with GLP-1RA and DPP-4i for metabolic resilience.
🔹 5. The “Beyond GLP-1” Frontier
Incretin-based evolution: Dual and tri-agonists (GLP-1 + GIP ± glucagon).
Amylin analogues (e.g., Pramlintide next-gen) improve satiety and body composition.
🔹 6. Hepatic Metabolic Modulation – A New Axis
Direct enzyme modulators: Target key hepatic enzymes controlling glucose flux.
Epigenetic regulators (miRNAs, sirtuins) restore insulin signaling at transcriptional level.
🔹 7. Adipokine Pathway Modifiers
FGF21 analogues, PPAR modulators, 11βHSD1 inhibitors – rebalance adipose signaling, promote lipid oxidation, and reduce ectopic fat.
🔹 8. Clinical Vision for the Future
The goal: “Multi-organ metabolic harmony.”
From “one drug, one target” → to “network modulation” across organs.
Early use of agents like Imeglimin + GLP-1RA + SGLT2i may preserve β-cell life and delay insulin need.
🧠 CME India Take-Home Message
🔸 The future of diabetes pharmacotherapy lies in bioenergetic repair, organ cross-talk modulation, and metabolic reprogramming.
🔸 Imeglimin marks the start of a new era — mitochondrial-centric diabetes therapy.
🔸 A combined approach across the gut–liver–muscle–beta-cell axis can potentially achieve durable remission.
https://t.co/WmAPzj373e