@PamelaMasonEP That is one of the reason I switched to stick the vein before cutting down to form the pocket. (Or do a venogram). Impressive lead positioning, but would have been easier from the right.
Scary Versacross transseptal case.On pulling down the sheath kept on sliding inferior hence aneurismal septum. Torking back to septum must have put pressure on AVN and complete AV block(13 sec-but felt longer). Baylis needle came to rescue.WM implanted fine.
@LukerJakob @EPeeps_Bot@narrowQRS@jeffrey_vinocur Is it due to that analyzer times off the (late) upright deflection. That may be the local activation, the rest of he complex could be far field- but downward defl. may be local activation as well-depending on the direction of the https://t.co/jZjPHw858z this true for the device?
@fvassallomd@bisbal_EP I agree,short sheet is less dangerous. I advance by ICE image alone. Trick is taking the curve at the iliac bifurcation, where it is easy to get confused. I like leaving a wire in the adjacent sheath and also a wire from the contralateral side. They show the way on ICE image.
@makkayadr@EPeeps_Bot Agree. All the less than useful algorithms to locate PVCs from left to right. In the end best bet is to map both side from he get go. True right sided are rare.
@KennethEllenbo1 I had a feeling that his pacing may be risky for complete AV block Patients. I tend to use a Biv can with RV lead backup when using a his lead. Agree, maybe LB pacing could be more promising, but needs similar evaluation for long term.
@grazianaviola One trick I am using for femoral venous catheter advancement is to leave the guide wire in the second sheath until I get the catheter up to IVC. This way if any resistance I can see if the catheter tracks the guide wire. Quicker than venogram. But one can only see perf on venogr
@OfSinus @EPeeps_Bot Let me guess, large chested female? They are notorious for monster vertical generator shifts on standing up. Coupled with sleeve release- see anchor not technique by Worley. Hope it helps.
Another case LV lead pulled back now target is occluded. Sleeve tied tight directly to the muscle but then turned to scar. Can't tie directly to the muscle with enough tension to pass tug test without causing necrosis then scar. Tie to the Knot. #EPeeps@narrowQRS@rdschaller
@JamesKnellerMD Agree. On the other Hand patient care does not stop at 5 pm. Also physicians tend to think of themselves as their own bosses, and just keep in exploiting themselves. Hence the high burnout rate. We have to yearn for better organized work, so life work balance is achieved.
A well-worn testing method would allow 10 times as many Americans to be tested for the coronavirus with only the resources available now. https://t.co/jwxM8RXk4n
Since we started using US Guided axillary vein puncture for CIED implantation people asked a lot about our workflow for these procedures. This is my humble contribution for this field.
#EPeeps#ultrasoundaxillaryfirst#POCUS#cardiotwitter#medtwitter
https://t.co/O9IhOJ2MxO
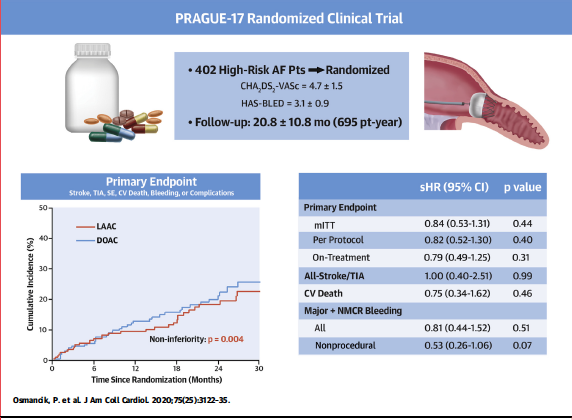
The Pivotal randomised PRAGUE-17 trial showing equivalence of LAAC with NOAC in high-risk AF patients published in @JACCJournals
https://t.co/Rbp1Icm63u
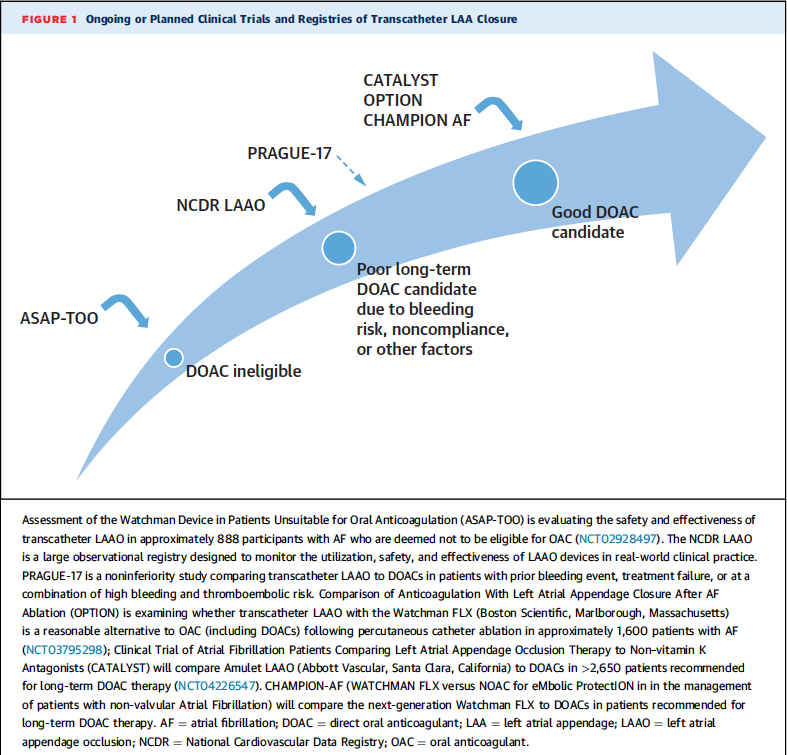
An excellent editorial by @docsaw puts it in context with previous and upcoming trials.