@MuzamilArshad18@LocasaleLab Cool man, go ahead and do that then! No one is stopping you - in fact we are all rooting for you to find novel paradigms beyond targeting 1-2 markers at a time. Show your results, get your funding, and do your trial. Until then - stop obsessing over theoretical limits of efficacy
Historical pattern in oncology: every advance (immunotherapy, ADCs, etc.) draws “it’s not that great” takes, even when data are unambiguous.
We need builders, not arsonists or contrarians. Stop tearing down; run the next trials, expand indications, iterate on resistance. 🚀 #ASCO26
@MuzamilArshad18@UGrewalMD@5_utr@TimothyJBrownMD None of us who do targeted therapy underestimate the ability for cancer to evolve - certainly multimodality approaches to maximize its use are needed. These are not reasons to abandon pursuits of targeted therapy in general like this gentleman routinely argues. Ludicrous.
Remarkable consistency across trials that >50% DLL3 expression is required for TCE monotherapy activity in NECs. How to evoke responses in lower expressors is our next challenge (?combinations, ADCs, others…). #ASCO26
ZG006- Phase II trial with trispecific T Cell Engager DLL3/DLL3/CD3 in NEC at @ASCO#ASCO26
ORR if DLL3 high at 30 mg 56%, DOR 11.7 months
🙌🏻Consistent - DLL3 works in NEC
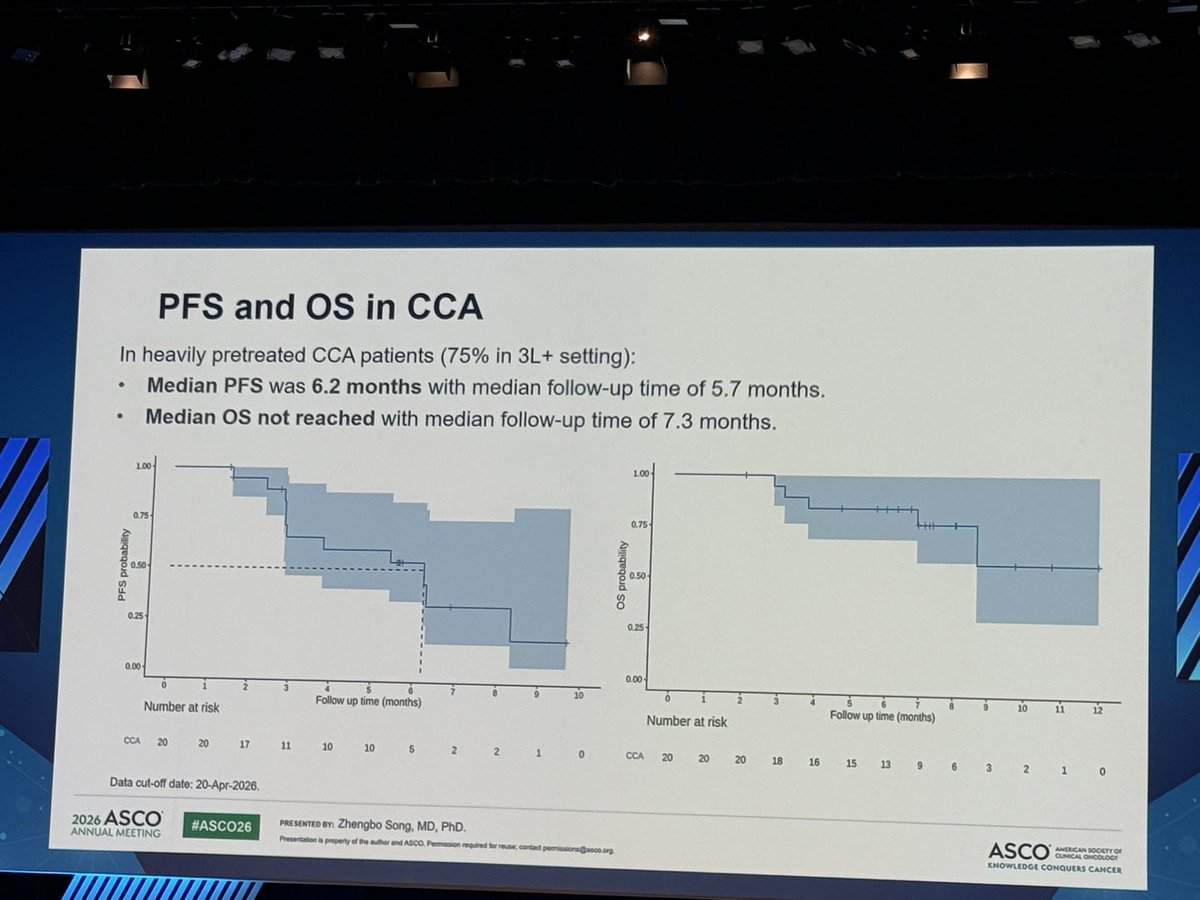
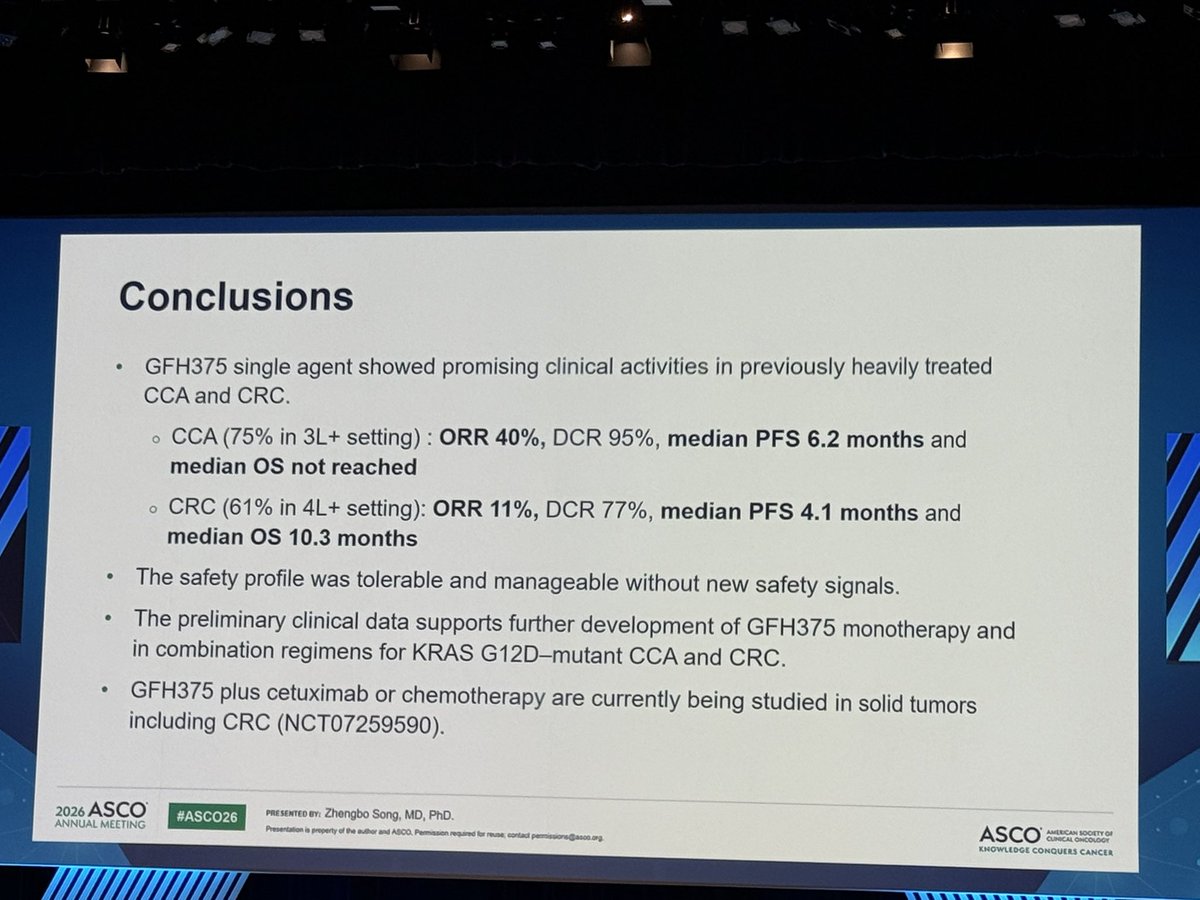
#GFH375 activity in heavily pretreated KRAS G12D–mutant cholangiocarcinoma/CRC #ASCO26.
CCA: 75% in 3L+; ORR 40%, mPFS 6.2 mo
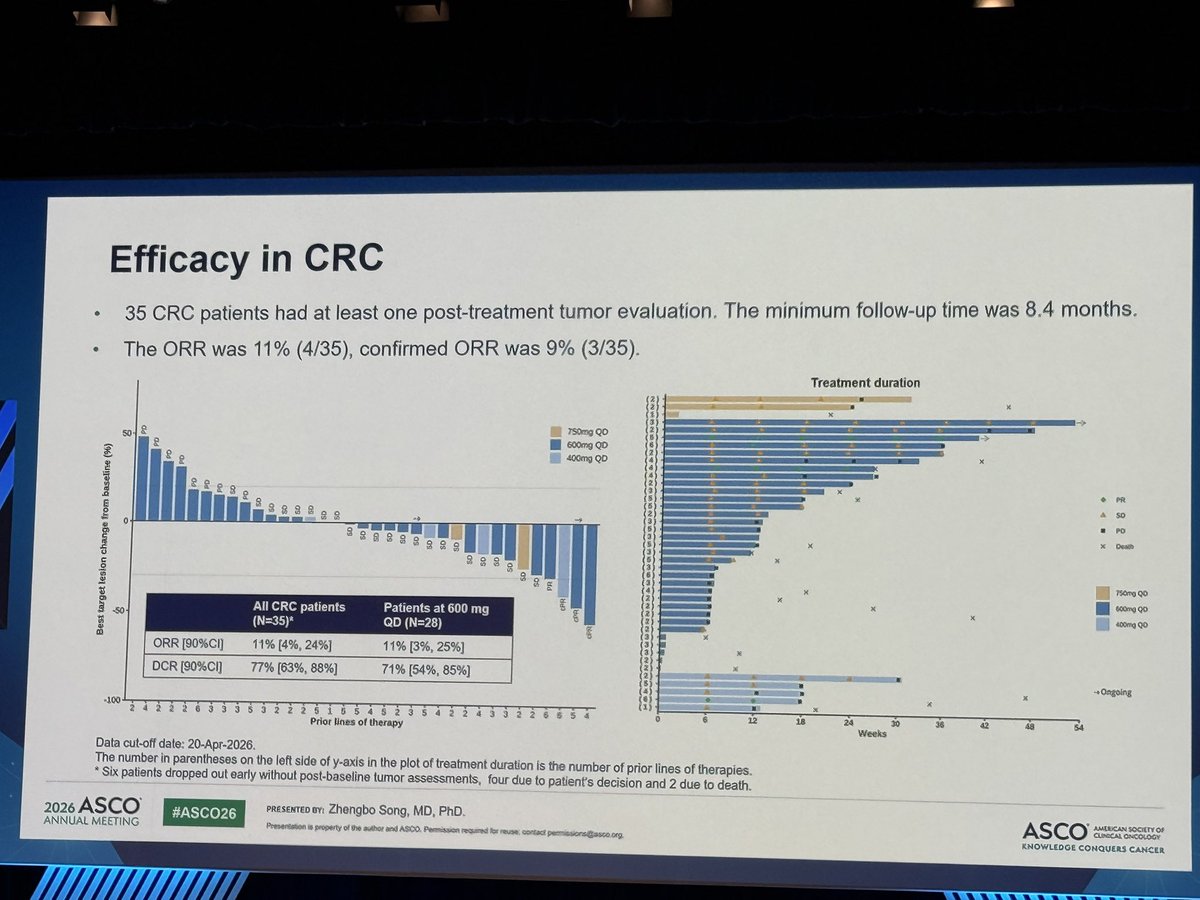
CRC: 61% in 4L+; ORR 11%, mPFS 4.1 mo
Safety: mostly GI, hematologic AEs and transaminitis; generally G1/2.
Early, but worth watching.
@venkmurthy@marklewismd Think these are mostly meant to be tongue in cheek, or some folks perhaps not focusing on the right takeaways. Agree with you p-value is only useful when assessing the right/meaningful endpoints and considering magnitude of benefit, which most would say this study did well!
@NiuSanford@UGrewalMD@OncoAlert Completely agree! 30% response rate in chemorefractory patients, for patients with locally advanced disease, can we do darax -> ablative RT if response? I am certainly going to try…
@mtymtyyanmaz@5_utr Ignore him. This gentleman has unfortunately lost the plot. The lorla benefit might be related to unreported oligomet RT? 😂😂😂 Feel sad for him typing out this thread in his basement!
@coffman_kelley@EileenMOReilly The time to radiographic response data presented doesn’t do this justice. I’ve seen pts feel better (and worse if held for tox) within 1-2 days. Really incredible!
A few butterflies🦋 before the #ASCO26 Plenary. #2025Plenary podium was unforgettable , but this seat is definitely more relaxed. Emotions are high for the PDAC and sarcoma presentations. If we can change practice in these recalcitrant diseases, anything is possible! 💜💜💜
Some key takeaways: this was a 2L study (~80% of pts with 1 prior line in advanced setting); RR ~30%, median time to response ~2 mo. We will need to contextualize this efficacy/safety data when offering to sicker pts with more heavily pre-treated disease.