Founder, MIT Sloan, coach, fmr Chief Med Officer & Medicaid med dir, Top Voice 4x, data nerd, digital health, MedEd, humanist, Tweets personal, RT🚫endorsement
@DocLauraLawler @freckledpedidoc @BetaMomma@drbatraneo@MAhealthforkids@mainlinehealth As doctors we must understand:
asymmetry of power/knowledge in the doctor-patient relationship
vulnerability of patients
the sacred trust they put in us by sharing their stories, bodies, hopes, fears, pain
An x-ray is not just an x-ray. Is someone’s body part
#medtwitter
@RepGregMurphy Second, it is deeply concerning you are not able to understand what this shows, to read the x & y axes correctly. Please read the reader corrections below the tweet for what the chart shows.
@RepGregMurphy Do you feel your being chosen by a medical school also was their wrong choice?
You left medicine. You are among the group in that chart, doctors that left clinical practice.
Of course, the Constitution does not prohibit simplification. (That is not what I said.)
I merely quoted the law on: authority over health is with the states in the Constitution.
If states agree, they certainly can collaborate.
A start up seeking to “solve” this would need to know the law prior to just assume.
My advice to any start up founder: do understand the legal/regulatory landscape.
https://t.co/EEl8q6LjZW
While I agree that the reframing is important, from a #data perspective. I wonder if some of the existing diagnoses will get lost because nobody will map the prior diagnostic terms to the current ones in the #EHR.
So much is getting automated and turning towards AI that getting down into the weeds of the data is essential to ensure that women’s health actually is “seen” by the system.
A medical school professor walks into clinic with her 12 year old son. He has 18 specialists. She does not fill out the intake form anymore. She hands the front desk a one-page medical sheet and says, "This is the current state of affairs," because the complexity will not fit in anything a clinic prints.
That is Kathleen Muldoon, a med school professor and the parent of a medically complex child. She and co-guest Jonathan Cottor came on the podcast to talk about what pediatric medicine misses when it treats the diagnosis as the whole job. Kathleen is the one teaching your future colleagues what humanistic, whole-person care looks like. She is also the one who gets up in the middle of the night to reposition her son, because he cannot move on his own.
Here is what your 15 minute visit does not see.
The alarms that go off all night. The cold mornings in Arizona when his whole body tenses and nothing moves the way it should, which changes his mood before you ever lay eyes on him. The communication device she has to fight for so people can finally hear that her son can answer his own questions when he is given the chance. The two siblings absorbing the labor and the mood of a household run on triage. The third grader asked at school whether his brother was going to die. The six months of logistical work it takes to arrange a single weekend away.
She has a spider web diagram she shows med students that maps all 18 specialties and how they interact, because none of them talk to each other. The diagram is not a curriculum exercise. It is the operating manual of her actual life.
We have built a pediatric system that treats medical complexity as a list of diagnoses to manage. The families managing those diagnoses are running a 24/7 operation with no shift change, no relief team, and a clinic visit that asks about A1c but not about whether anyone in the house has slept. The intake form has a field for allergies. It does not have a field for "the parent across from you has not slept through the night in years."
The reframe worth bookmarking: care is not just clinical, it is relational. When you care for the caregiver, you are caring for the whole family. In a 15 minute visit, that is three questions. Do you have respite care. How do you care for yourself. What would make it easier for you to keep doing this safely.
Those three questions are the cheapest, highest-leverage intervention in pediatric medicine that almost no chart prompts you to make. They take under a minute. They cost nothing. They tell the family across from you that the person doing the most work in their child's care, the one with no medical license and no shift end, has finally been seen by the system that prescribed it.
Listen to the full conversation on The Podcast by KevinMD. Link in the replies.
Which of those three questions have you been avoiding asking, because you are afraid of the answer? #ThePodcastbyKevinMD
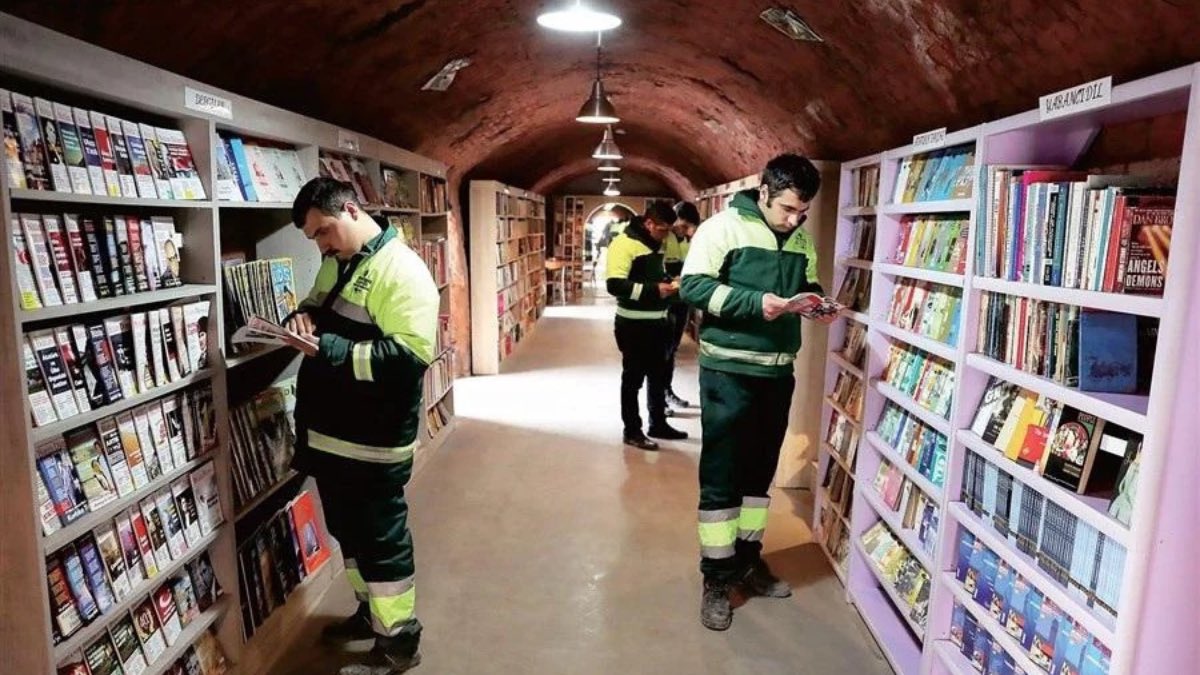
A binman in Turkey’s capital found a bag of thrown-away books on his rounds and couldn’t bring himself to take it to the dump. He kept it. Other workers started doing the same. The pile has now grown into a public library of over 9,000 books, run by sanitation workers, in an old brick factory.
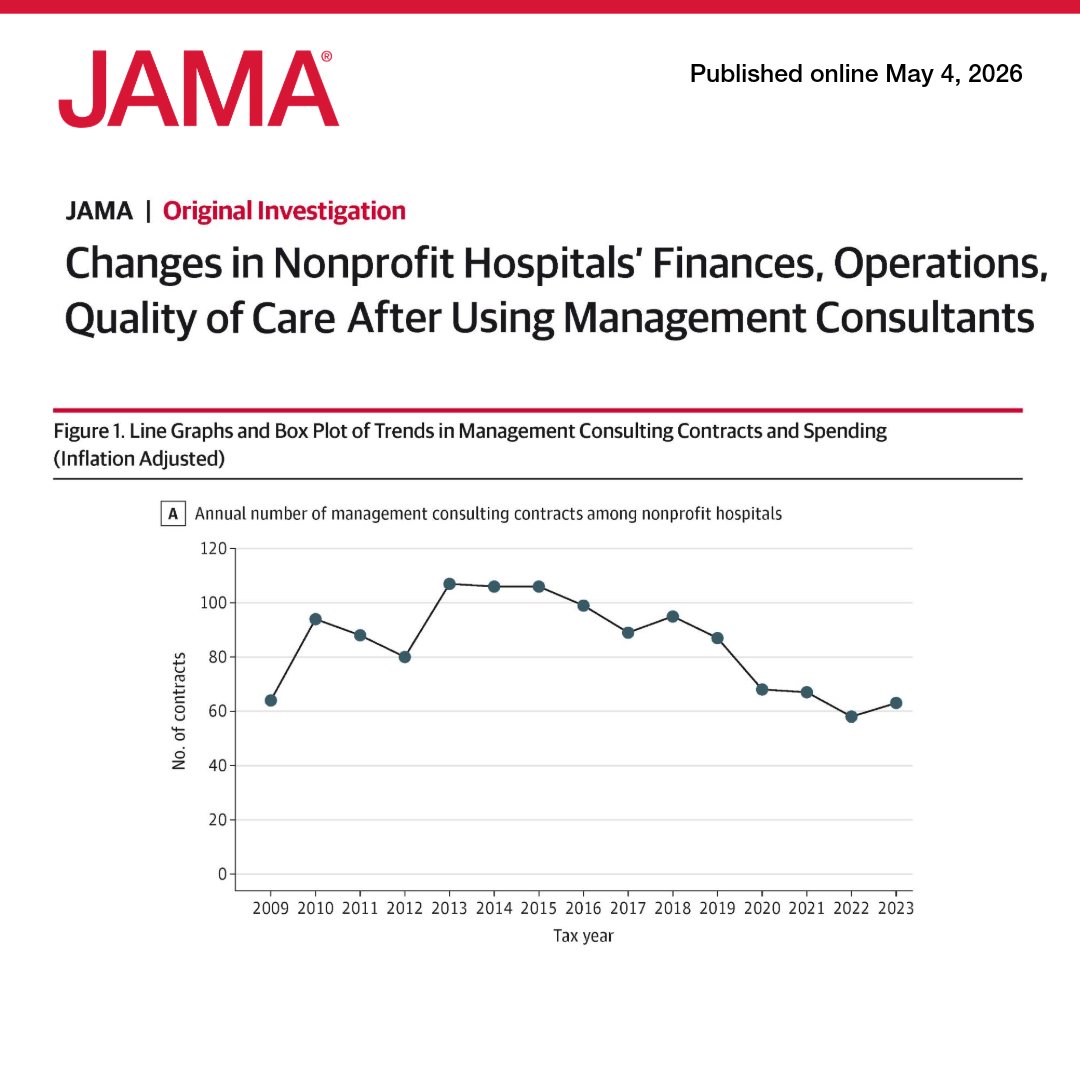
US nonprofit hospitals spent $7.8 billion on management consultants from 2009 to 2023, but contracts were not associated with meaningful changes in finance, operations, or quality of care. 🧵
https://t.co/QQswMYxrG8
@Hemida_MD@SpringerNature Meanwhile, unless I can ask a colleague to do me the favor of review, if, as a guest editor, I just use the system’s recommended reviewers, I need to invite 50+ or 100+ to get three to agree and to complete it
Twenty years ago, longevity medicine did not have a name. No standards, no curricula, no consensus on what counted as evidence.
Today, Advanced Research Projects Agency for Health (@ARPA_H) has committed $144 million through its PROSPR program to develop therapeutics that target the biology of aging directly. The @xprize Healthspan competition is mobilizing global talent. Governments from Saudi Arabia to the U.S. are funding aging research at unprecedented scale. The field has reached an inflection point.
The field has reached an inflection point. The people building it are gathering in Cambridge on May 26 and 27 for the Aging Code Summit, part of the inaugural Boston Tech Week. I'm speaking on Day 2.
A few of the conversations I'm most looking forward to: @manoliskellis (MIT) on the computational biology of aging Li-Huei Tsai (The @MIT_Picower Institute for Learning and Memory) on the latest in neurodegeneration Kristen Fortney @kpfortney (@bioagelabs) on translating aging biology into therapeutics Sharon Rosenzweig-Lipson (@lifebiosciences) on the science behind a leading longevity company @mahdi_moqri (@agingbiomarkers Consortium) on where aging clocks are headed Amy Proal, PhD @microbeminded2 (@polybioRF Research Foundation) on chronic infection in aging Saranya Wyles, M.D., Ph.D. @drwyles_derm (Mayo Clinic) on regenerative dermatology and skin longevity Jens Eckstein @AkikoaCom (Hevolution Foundation @hevolution_f) on capital meeting the science. My Day 2 talk focuses on evidence-based best practices in longevity medicine, the framework I've been developing across clinical practice, Harvard Medical School teaching, and advisory work with longevity organizations worldwide.
The question I keep returning to: which interventions actually deliver outcomes, and how do we tell. Day 2 also features the pitch competition, where top seed and Series A companies compete for a one-year residency at The Engine, MIT's tough-tech platform and one of the most consequential launchpads in longevity right now.
If you work where this field is being built, you should be in this room. Register: https://t.co/nMEWFICY9F
Joining an extraordinary faculty including Christin Glorioso MD PhD @DrGlorioso (NeuroAge Therapeutics @NeuroAgeTX), @JamieHeywood (@AldenScientific), Fiona Miller (@quadrascope), @Dr_RayMak, José Navarro Betancourt, MD, PhD, Justin Taylor, Noriko Yokoi, Ph.D., Daniel Dacey, SpringBehrouz, Raghav Sehgal, PhD @rv_sehgal, Jay Luthar, MD, DipABLM, @HillaryLinMD, Umbereen S. Nehal, MD, MPH, MBA @usnehal, @tomzuber, Robin Mansukhani, Fernanda Cerqueira, David Hall, Yeh-Chuin Poh, Salah Mahmoudi, and @RutaLaukien
Updates at: https://t.co/gEHdRRxB35
More at https://t.co/onwb1qIVVy #BostonTechWeek #LongevityMedicine
In healthcare, no amount of personal wellness practices can substitute for appropriate staffing, humane scheduling, efficient clinical workflows, adequate administrative support, or a culture of psychological safety.
@LorickFoxPA@StuartBlitz The answer is not based on urban/rural practice differences but the 10th amendment and federalism: powers over health & safety not explicitly given to the federal gov’t reside with states. Hence state medical boards, state dept of public health, state health dept, Medicaid, etc.
@LorickFoxPA@StuartBlitz I’m also not on board (pardon the pun) on different standards of care. Yes, of course there are different ground realities by setting. That, though, also is true between NYC boroughs & neighborhoods.