@drjohnm Brilliant trial and Prapa's vision has always been incredible. There was so much I learned about Cryo and workflow from Prapa post AVATAR era (even when we were looking for electrical confirmation). Not mapping PVs during ablation was politically unpalatable to the reviewers.
In March, an Imperial College team published results of AVATAR--a 3-arm trial comparing standard CB AF ablation, AAD, and CB ablation *Without* confirming PV isol
Guess what? There were no diff in symptomatic AF bw the two ablation approaches! Both better than drugs
https://t.co/9wELERP8ET
Why has no one talked about this story? No media coverage.
It's totally provocative b/c it challenges the current practice of confirming PVI . #EPeeps
cc @bordistef@RolandTilz@bogdienache@ftrae@DhirajGuptaBHRS@EPWaveDoc@DrRoderickTung@LuigiDiBiaseMD
@OrthopodReg There are many complexities to how healthcare functions in Australia with fractional contracts and much more substantial private overlay. The market for this in some specialities is >50%. It's difficult to compare the two. At least some movement here in UK.
Great great stuff from my adopted homeland, Australia kept it tight and Travis smashed it home despite the conditions, despite the crowd and despite the expectations. 🇦🇺
@UKGastroDr @FPARCP Perhaps the best approach is to remove the word physician from the title altogether when one has no medical degree. Maybe just medical assistants.
Most ECGs are printed on paper 📜📜
Thus not suitable to train AI-ECG models
So we developed an automated ECG digitisation algorithm to extract digital ECG signals 🖥️🖥️
Well done @DrKiranPatel1@arunsau_@NikeshBajaj et al
@ImperialNHLI@ImperialEP
https://t.co/avqxI9Np5y
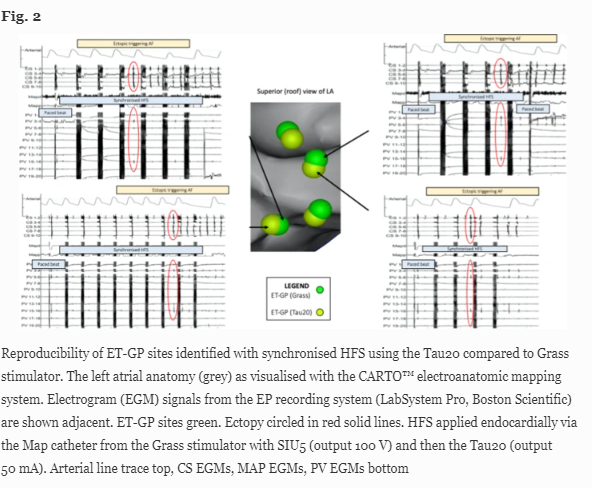
What are the immunohistochemical characteristics of atrial sites that trigger atrial arrhythmias in response to high-frequency stimulation?
Our paper now out in Europace.
Amazing work by @DrMYKim and colleagues @ImperialNHLI@ImperialEP - well done!
https://t.co/CUfuIUYEq4
@javadm20 At our centre, we all pace the phrenic high up in SVC for right sided PVs with a quad. Then pace with lower output, establish a threshold and go slightly above. During the freeze, one hand over abdomen and stop at any sign of loss / attenuation. Right lower PV before right upper.