ASCO2026: Asymptomatic brain met EGFR/ALK NSCLC any benefit upfront cranial RT on this Randomized trial?
- Upfront RT ↑↑ brain control, no benefit PFS, OS
- Selection criteria high risk (e.g. larger size) for upfront RT is key
https://t.co/1CM31nbxeL
Presented at #ASCO26:
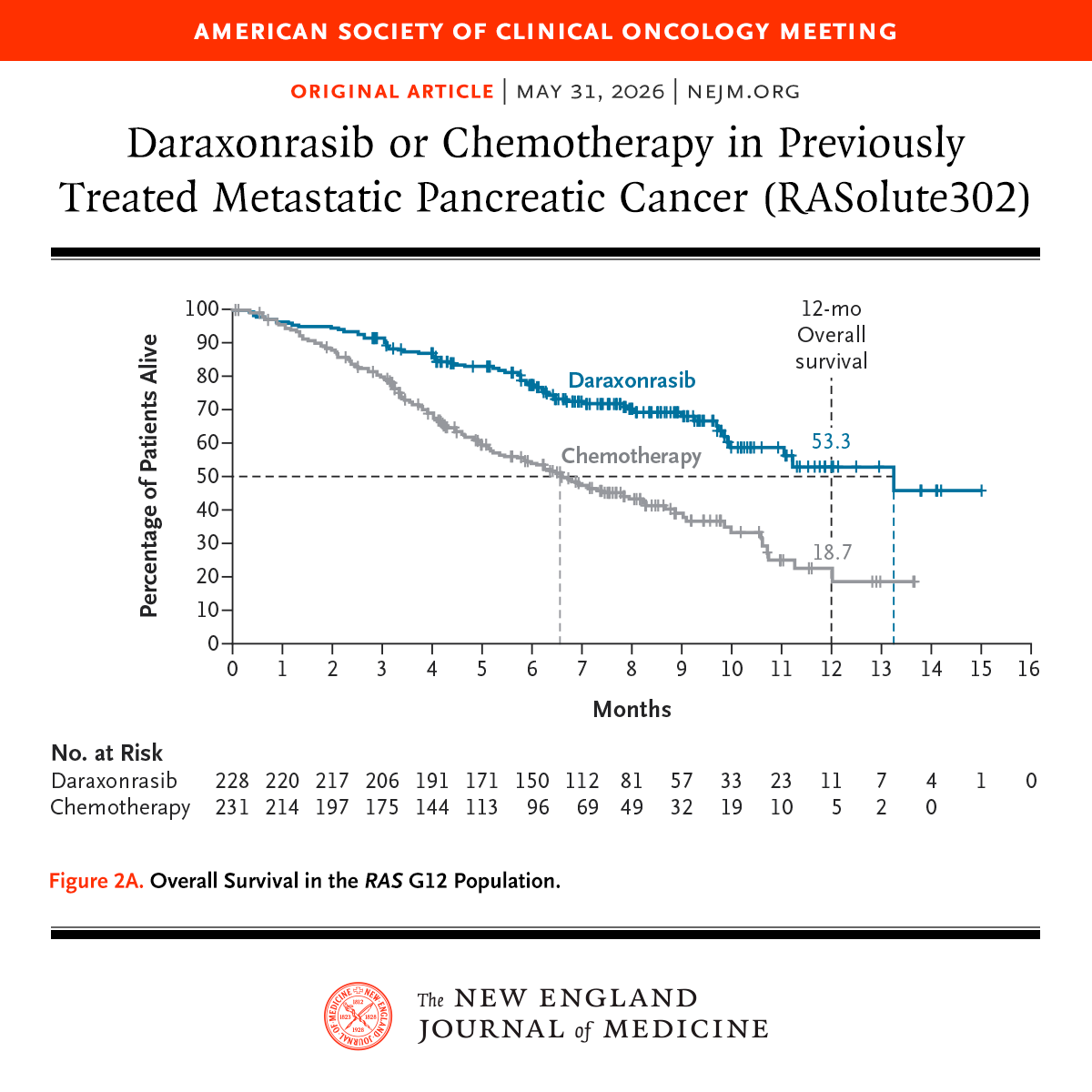
Among patients with previously treated metastatic pancreatic ductal adenocarcinoma, the RAS(ON) inhibitor daraxonrasib led to significantly longer overall survival and progression-free survival than chemotherapy. Full phase 3 RASolute 302 trial results: https://t.co/xwLWBZYRzq
@ASCO
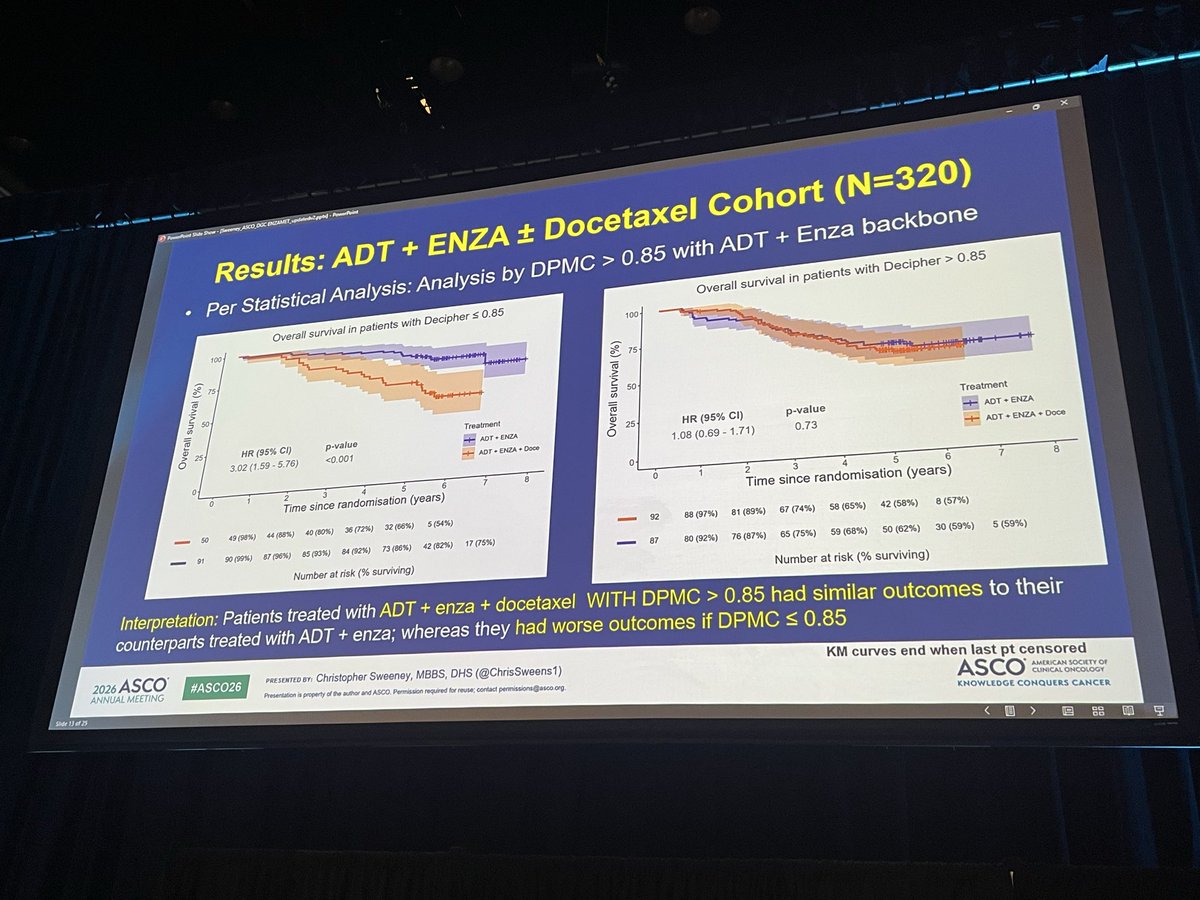
@chrissweens1 presents level 1B evidence from ENZAMET suggesting Decipher GC >0.85 may identify pts deriving benefit from docetaxel intensification alongside ADT + enzalutamide, while no clear benefit signal was observed for GC ≤0.85.
#ASCO26 #ProstateCancer
@O@OncoAlert@ASCO@OncBrothers
2/n #ASCO26
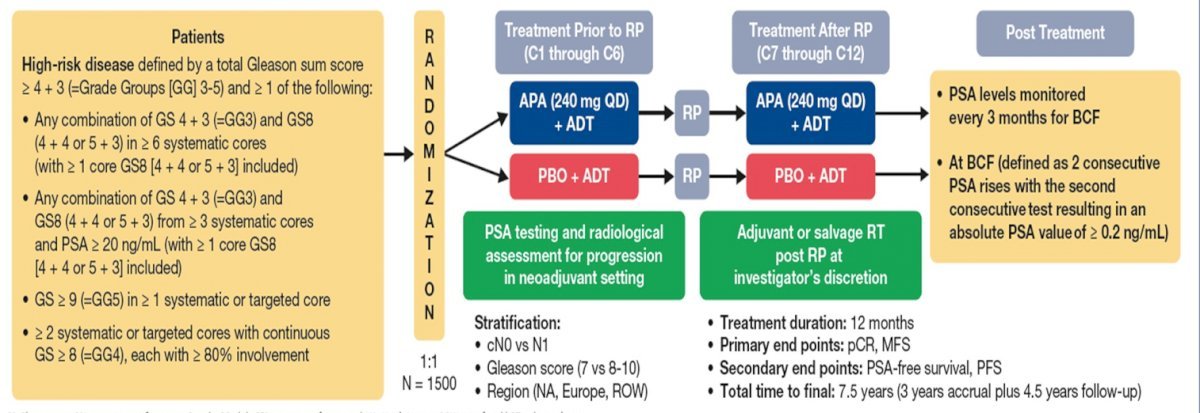
The design.
Peri-operative ADT (12m) + RP vs
Peri-operative ADT+Apa (12m) + RP
Robustly blinded, placebo controlled.
Some may criticize that the SOC is not RP+ADT, but simply RP, but others may state this raises the bar to show benefit of apalutamide.
@WallisCJD@HimanshuNagarMD@ChapinMD@CaPsurvivorship@wandering_gu
🚨🚨 ASCO 2026 Final Results Randomized trial resected brain met Brachytherapy vs Post-Op SRS🚨
- Incredible Surg Bed Control with Brachy (↑↑OS as well)
- Surg bed recurrence 12% SRS vs 1% GammaTile
Definitive Radiotherapy to the Primary Tumor in Stage IV NSCLC: A Consensus Statement From the International Association for the Study of Lung Cancer Advanced Radiation Technology
Subcommittee
https://t.co/iPbTjLcCLi
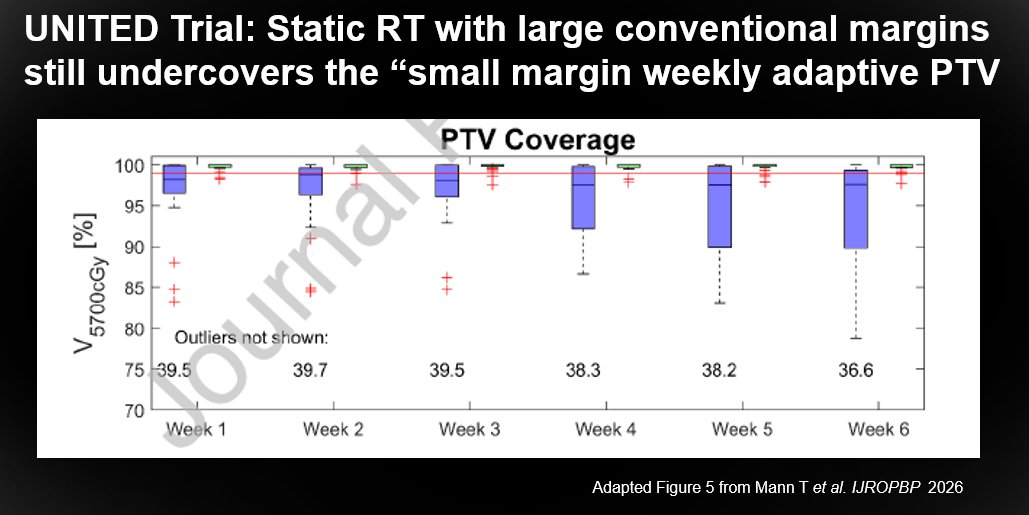
Team @Sunnybrook just published in the @IJROBP a wonderful secondary dosimetric analysis of the UNITED Trial on MRgRT for #GBM. I think Figure 5 from the manuscript makes a compelling case for change. It suggests that static radiotherapy, even with large conventional margins, under‑covers the small adaptive PTV.
https://t.co/5P29k51hPt
@mr_linac, @jaydetsky@SahgalArjun
ARTO Trial: Long-term overall survival analysis from a randomized phase II trial testing the benefit of SBRT addition to abiraterone acetate in oligometastatic #CRPC patients. Presentation by @GiulioFrancoli1@AOUCareggi. #GU26 written coverage by @RKSayyid@UAUrology > https://t.co/kWzd2v266x @ASCO
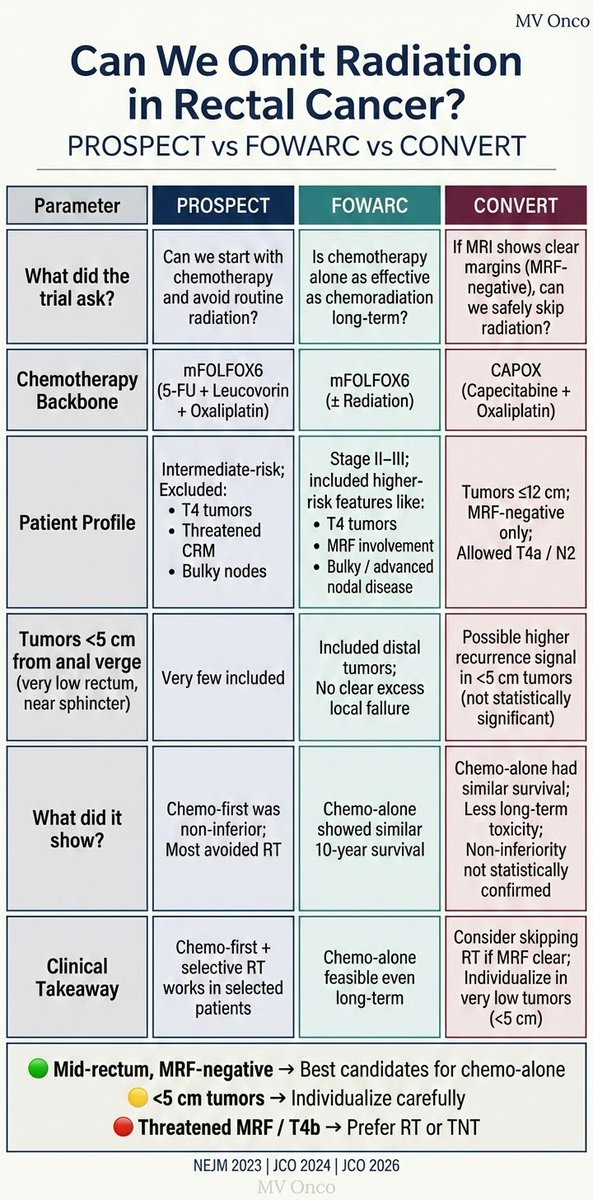
🚨CONVERT🚨
LARC with clear MRF
N=663
🔎nCAPOX x 4 vs. nCRT
LRRFS: 96.3% vs 97.4% (non-inf not established)
DFS3: 89.2% vs 87.9% (p=NS)
OS3: 95% vs 94% (p=NS)
🔑Another important study for LARC! This should be viewed in the greater context of:
❓How can we best balance cancer control and long term quality of life/function for our patients
- sometimes that is RT omission
- sometimes that is organ preservation
- sometimes TNT remains ideal
https://t.co/3sDwATrNQE
@ASCO@JCO_ASCO
New in the #RedJournal: replanned TROG 12.01 unilateral cases to define guidelines for unilateral RT planning with maximal midline and contralateral sparing. @TROGfightcancer#RadOnc#HNcsm https://t.co/yvE7RTRk3A
📃PSMA PET after RT ≠ straightforward.
Inflammation, fibrosis & PSMA flare can mimic progression, and quantitative PET biomarkers still lack validation.
👏 Congrats to all authors, especially Victoria Vera (part of her PhD thesis)
🔗 Free access: https://t.co/u7gxFLKoxf
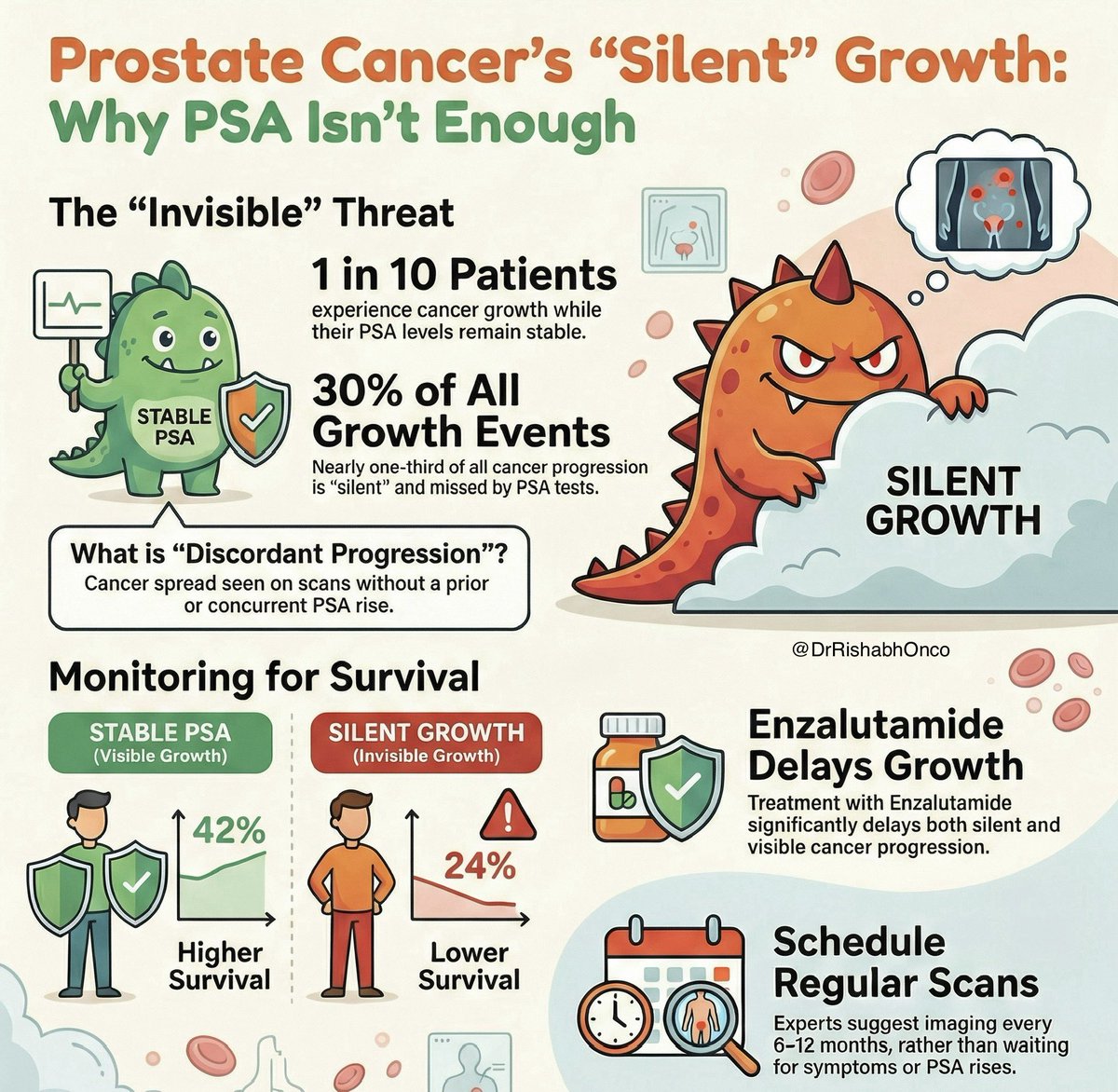
🔍 PSA can stay quiet while cancer progresses.
New ENZAMET post-hoc analysis shows radiographic progression without PSA rise in mHSPC is real, common, and dangerous.
🧪 Study essentials
•Retrospective analysis of ENZAMET (ANZUP 1304)
•n = 1125 mHSPC patients
•Enzalutamide vs standard NSAA ± docetaxel
📊 Key findings
•Discordant progression (DP) in 10% overall
•Accounts for ~30% of all progression events
•5-yr OS: 24% (DP) vs 42% (other progression)
•Enzalutamide delayed DP (HR 0.66) and OP (HR 0.37)
🧠 Clinical takeaway
•PSA alone is not enough
•DP carries worse survival irrespective of treatment
•Supports regular scheduled imaging, not only PSA-triggered scans
⚠️ Why it matters
•Silent radiographic progression risks late treatment switch
•Highlights biological heterogeneity in mHSPC
📌 Bottom line
In mHSPC, no PSA rise ≠ no progression.
Imaging needs to stay proactive.
🔖 Save for clinic
📖 Full paper in comment ⬇️
#OncoTwitter #MedTwitter #ProstateCancer #mHSPC
@OncoAlert@myesmo@esmo_open@asco
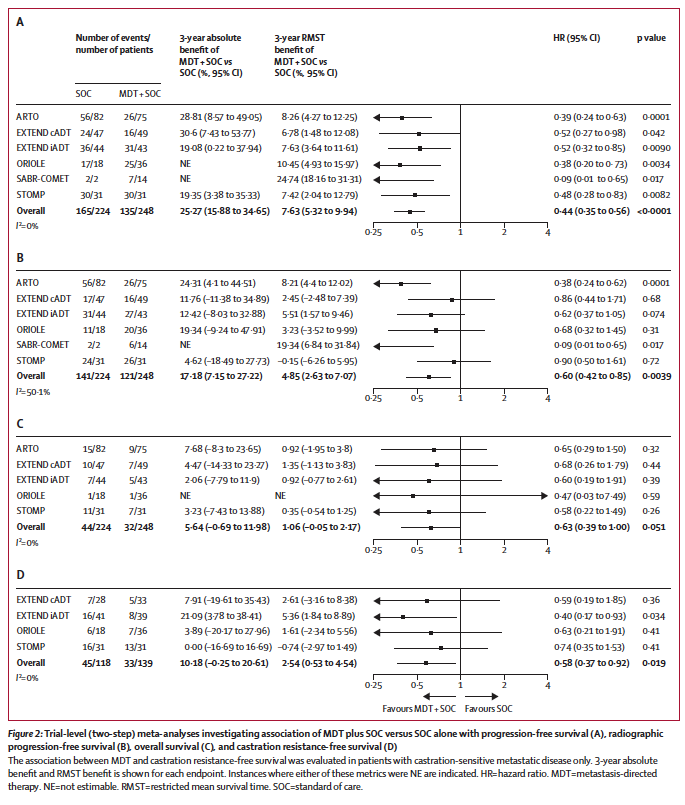
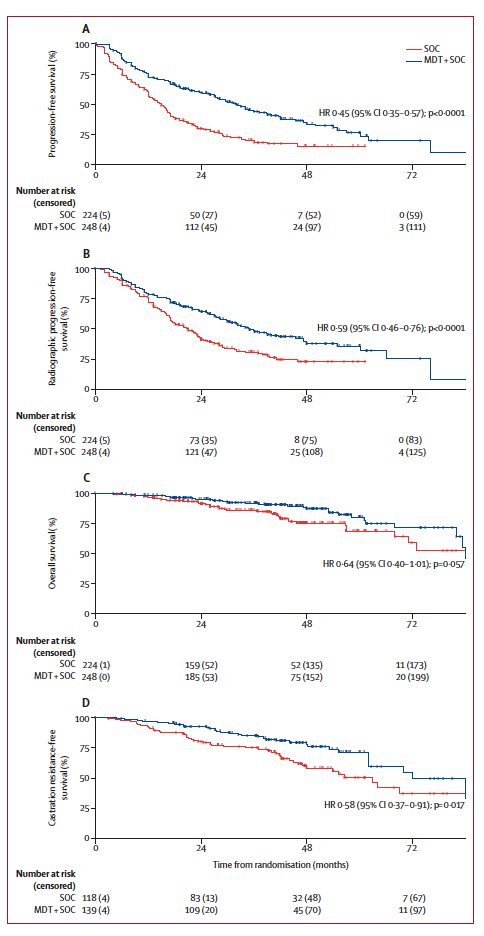
🚀 MDT in oligometastatic #ProstateCancer 🚀
👉WOLVERINE IPD meta-analysis in @TheLancetOncol
🧪 7 randomized trials, 574 pts
📉 MDT → ↓ progression, ↓ radiographic progression, ↓ time to CRPC
🔁 Consistent benefit across SOC (obs, ADT, ARPI)
🛡️ Low toxicity, short treatment courses
⚖️ OS not definitive; but this is the strongest evidence yet to integrate MDT
👏 @ChadTangMD@piet_ost
🔗 to study https://t.co/OtIHw4RGgV
🔗 to editorial https://t.co/aeWi3Wx0ms
@PCFnews@urotoday@UrologyTimes
Hot off the presses, ReCOG consensus statement endorsed by multiple Rad Onc societies now in @TheLancetOncol. Major step forward for advancing reirradiation. Congrats to authors, in particular @DrKCParadis, @ChuckMayoPhD, @elizapowerpuff.
@UMichRadOnc.
https://t.co/tJqsL28ltz
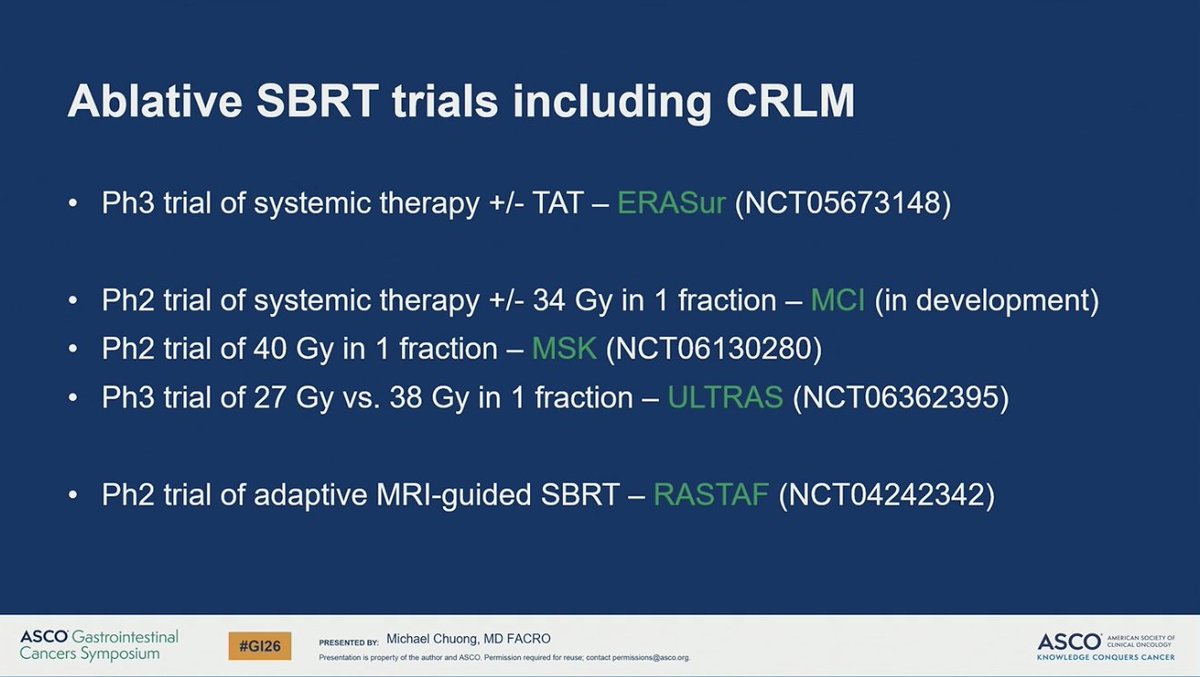
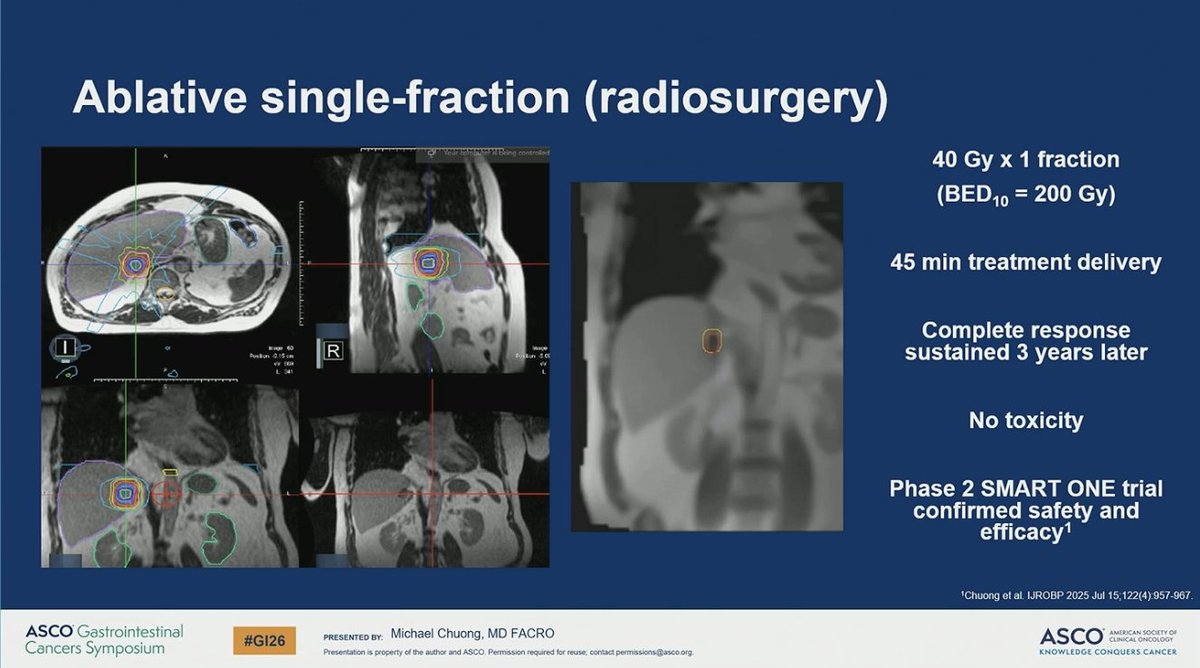
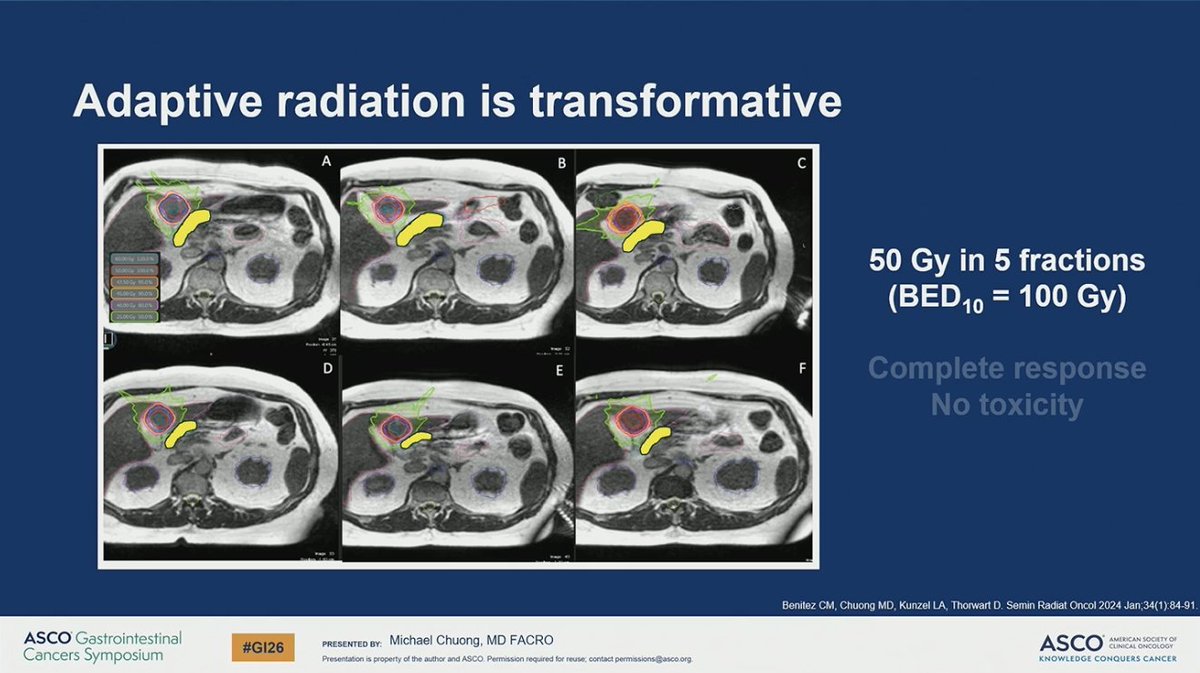
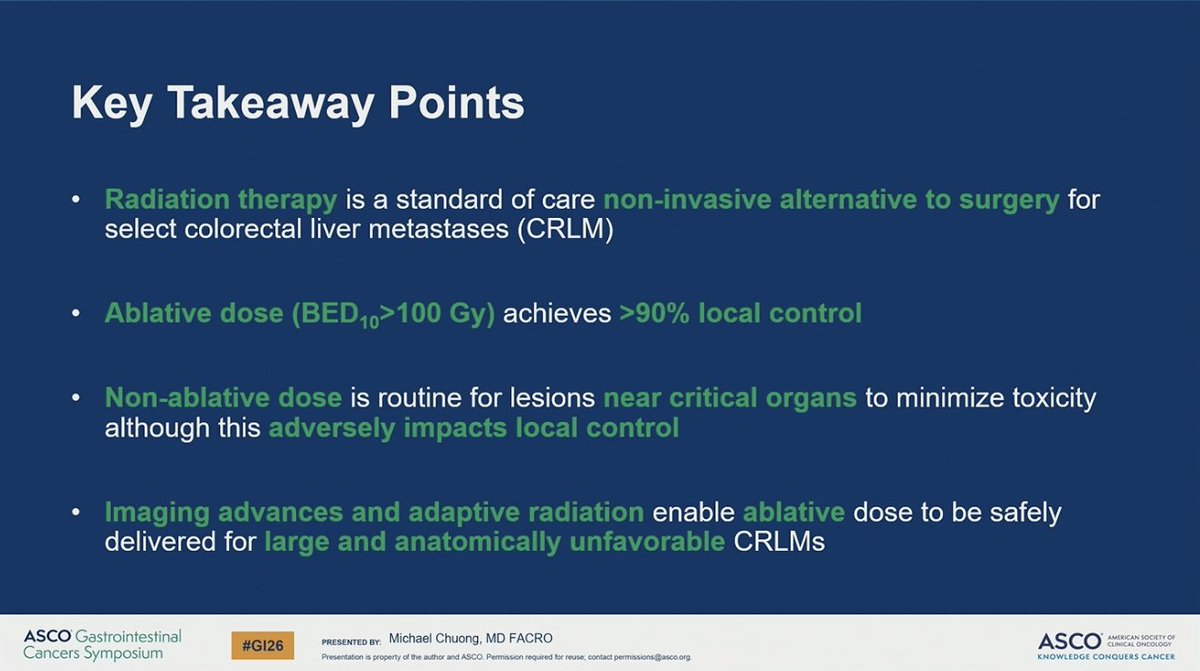
Great presentation on advancements in RT for liver metastases.
Ablative RT can be curative, non-invasive, & efficient.
No better person than @MikeChuongMD to highlight the evolution & potential of innovative RT technologies in this space. #GI26
Our new editorial is live! 📢
PFS & OS undervalue SABR in oligoprogression trials.
Focus on TTF, TTNT, and QoL instead—highlighting SABR as a repeatable strategic ally to systemic therapy.
👉 https://t.co/TH7FHQhYnd