An incredibly touching & thoughtful #ASCO26 Presidential Address from @ASCOPres Dr. Eric Small. Grateful to him for sharing a tremendously painful personal experience — which he has in turn transformed into a brilliant set of initiatives for @ASCO. Looking forward to the special session he has crafted on Monday featuring @crisbergerot, @KimmieNgMD, De. Irene Su & Dr. Tara Henderson.
PEAK-1 highlighted as a #OncoAlertTopTweet for Day 3 of #ASCO26. 🚨
@ASCO@OncoAlert
Important phase 3 trial-in-progress in advanced clear cell RCC after prior immunotherapy — a setting where better post-IO strategies are urgently needed. 🧬
Key design points:
✅ Casdatifan, a selective HIF-2α inhibitor, is being combined with cabozantinib
✅ Randomized, double-blind global phase 3 study vs placebo + cabozantinib
✅ Primary endpoint: PFS by blinded independent central review
This trial may help define whether HIF-2α inhibition can improve the post-IO sequencing landscape in #KidneyCancer. 🎯
@DrChoueiri@montypal@DrRanaMcKay@crisuarez08@tompowles1@AUC3_Official
#ASCO26 #RCC #GUOncology #OncoAlert
#ASCO26 GU Oncology Spotlight 🚨
🔬 Abstract 4521 | CaboNivo in non–clear cell RCC
Final results of phase 2 cabozantinib + nivolumab in patients with non–clear cell renal cell carcinoma
Presented by Darren R. Feldman, MD
@ASCO@OncoAlert
Important final dataset in a difficult RCC space.
Non–clear cell RCC represents a biologically diverse group of kidney cancers, often with fewer prospective data and historically poorer outcomes than clear cell RCC.
🔵 Study design
Investigator-initiated phase 2 study:
➡️ cabozantinib 40 mg daily
➡️ nivolumab 240 mg q2w or 480 mg q4w
Cohort 1 included:
• papillary RCC
• FH-deficient RCC
• unclassified RCC
• translocation-associated RCC
Chromophobe RCC was evaluated separately and closed early for inefficacy.
🟢 Final efficacy signal
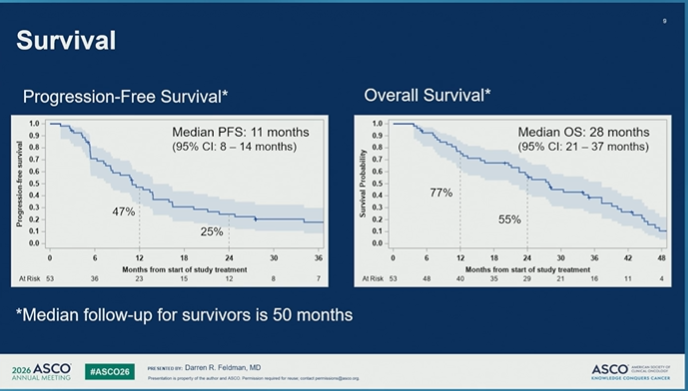
With longer follow-up of ~50 months, CaboNivo reaffirmed antitumor activity in non–clear cell RCC.
In cohort 1:
• N = 53
• PR/CR: 43%
• median PFS: 11 months
• median OS: 28 months
Responses were seen across several non–clear cell histologies, with a particularly notable signal in FH-deficient RCC:
➡️ 7/8 patients had an objective response.
🔵 Why it matters
Non–clear cell RCC is not one disease.
Histology matters.
Biology matters.
And prospective treatment data remain limited.
This final analysis supports cabozantinib + nivolumab as an active regimen for selected patients with non–clear cell RCC histologies, especially papillary, FH-deficient, unclassified, and translocation-associated disease.
🟠 Safety
Toxicity was consistent with known cabozantinib + nivolumab profiles.
Grade 3/4 treatment-emergent AEs occurred in a substantial proportion of patients, and discontinuations due to AEs occurred with cabozantinib, nivolumab, or both.
So this is active therapy — but not low-burden therapy.
🧠 My take
CaboNivo is one of the more clinically useful prospective datasets in non–clear cell RCC.
The key message is not “treat all non–clear cell RCC the same.”
It is:
➡️ use histology
➡️ recognize biologic subgroups
➡️ avoid assuming clear-cell algorithms fully apply
➡️ consider CaboNivo as a treatment option where prospective evidence supports activity
➡️ continue building trials specific to rare RCC subtypes
For non–clear cell RCC, better classification is the beginning of better treatment.
#ASCO26 #GUOnc #KidneyCancer #RCC #NonClearCellRCC #PapillaryRCC #FHdeficientRCC #Cabozantinib #Nivolumab #PrecisionOncology
@OncLive@TargetedOnc@CancerNetwrk@ASCOPost@ecancer@VJOncology@curetoday@JCO_ASCO
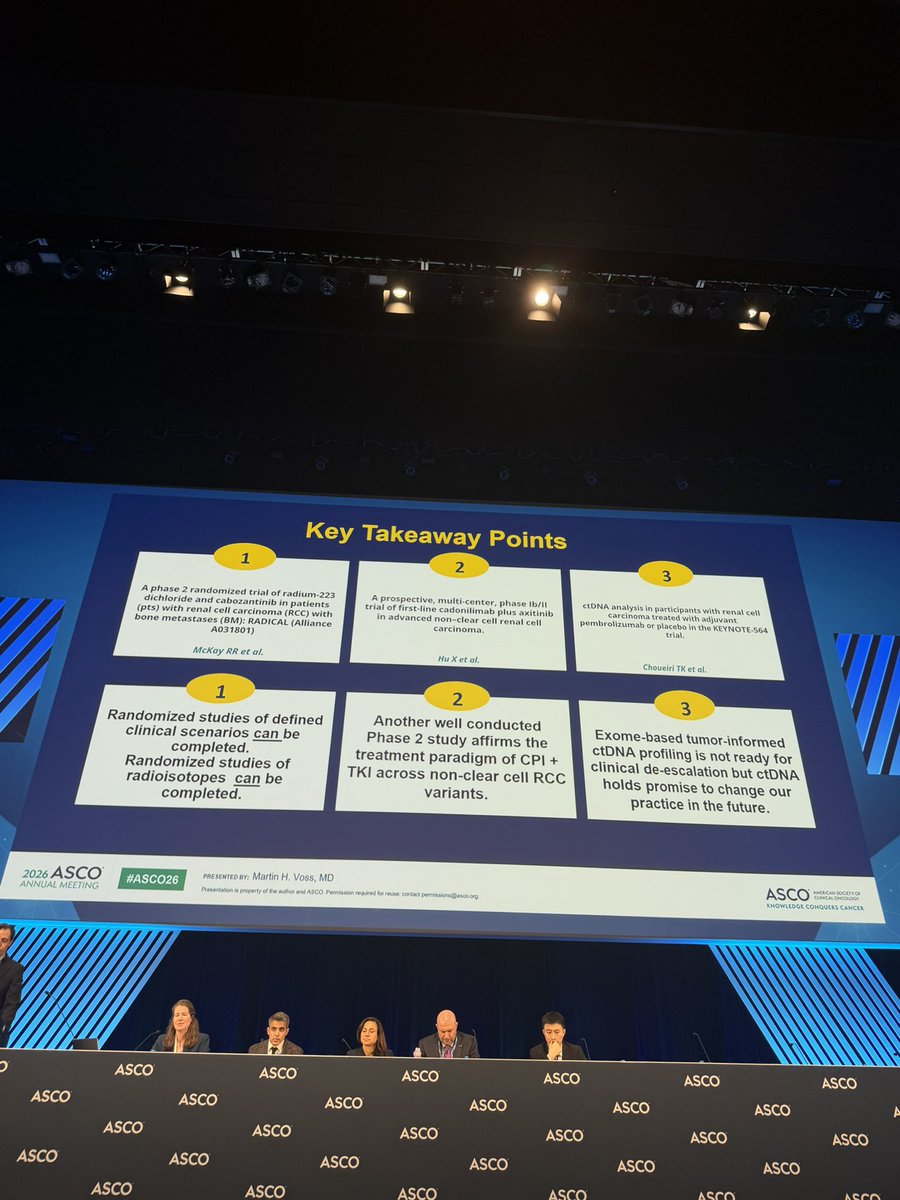
🟠 #ASCO26 GU — Kidney Cancer discussion
@ASCO
Abstracts 4500, 4501 & 4502
Discussant: Martin H. Voss, MD
“Is the Best Yet to Come in Kidney Cancer?”
@ASCO@OncoAlert
Three kidney cancer abstracts, three different clinical questions:
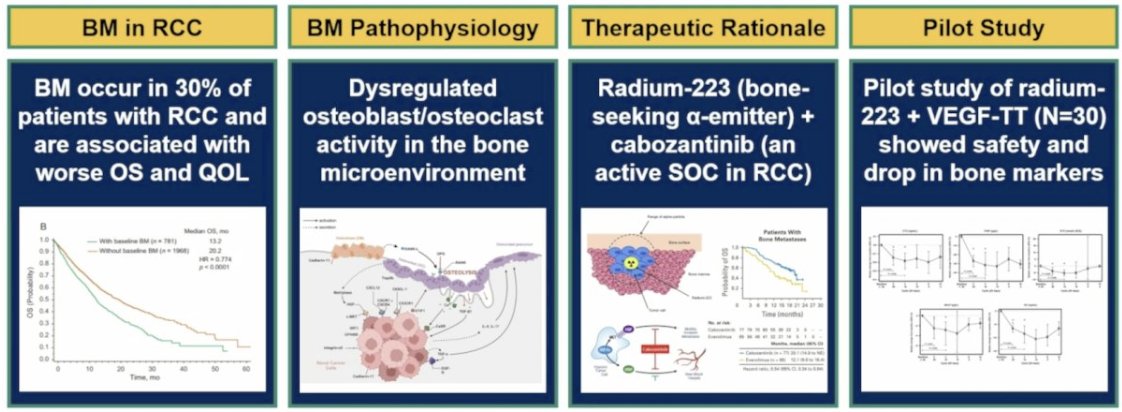
🟠 RCC with bone metastases
🟠 Non-clear cell RCC
🟠 ctDNA in adjuvant clear-cell RCC
Together, they highlight where kidney cancer is moving — and where the evidence is still catching up.
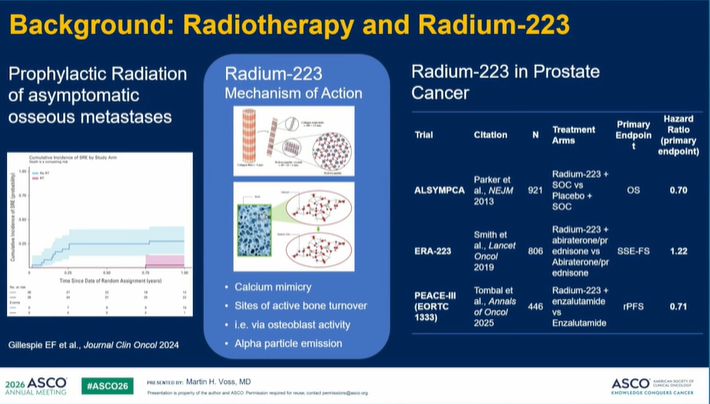
Abstract 4500 | RADICAL / Alliance A031801
Radium-223 + cabozantinib in RCC with bone metastases.
Key message:
➡️ No improvement in SSE-free survival
➡️ OS curves appeared to diverge after 1 year
➡️ Safety was manageable
➡️ Low on-study SSE rate limited interpretability
➡️ Differences in cabozantinib exposure may have contributed
My take:
A rational bone-directed combination did not translate into a clear clinical endpoint benefit.
For now, this should not change routine practice, but it keeps the question alive:
How do we better treat bone-dominant RCC?
Future work may need better patient selection, bone imaging, biomarkers, and newer radioligand strategies.
Abstract 4501 | Cadonilimab + axitinib in advanced nccRCC
A prospective phase Ib/II signal in a rare, heterogeneous disease space.
Key message:
➡️ ORR 51.6% in phase II
➡️ DCR 96.8%
➡️ Median PFS 14.2 months
➡️ Responses seen across several nccRCC histologies
➡️ Tolerability appeared manageable despite dual checkpoint + TKI targeting
My take:
This is encouraging, but not practice-changing yet.
The important point is broader:
Non-clear cell RCC should not remain an evidence-poor space.
These data support continued prospective testing of IO/TKI strategies across nccRCC, ideally with histology-specific and biomarker-enriched approaches.
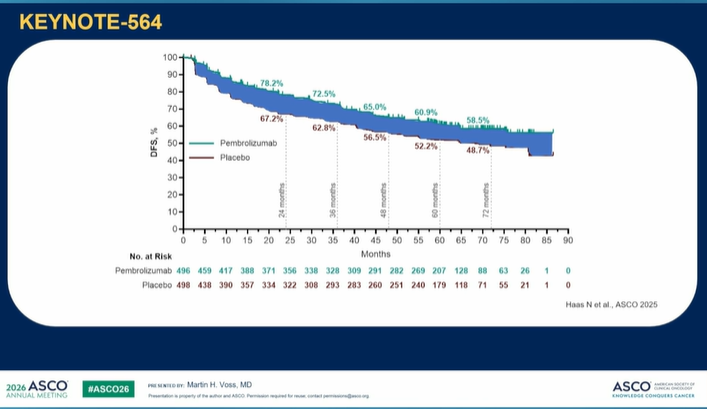
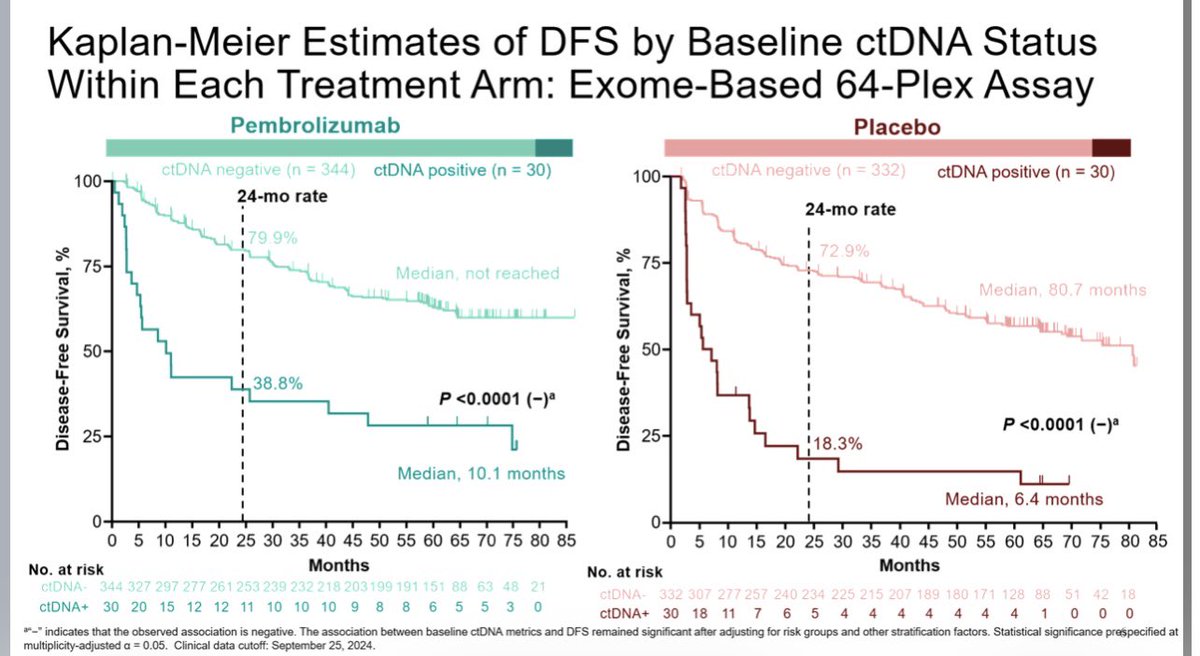
Abstract 4502 | KEYNOTE-564 ctDNA
ctDNA in adjuvant RCC after nephrectomy.
Key message:
➡️ Baseline ctDNA positivity was associated with worse DFS
➡️ ctDNA clearance was higher with pembrolizumab
➡️ Specificity was high
➡️ Sensitivity was low
➡️ Pembrolizumab benefit was observed regardless of baseline ctDNA status
My take:
ctDNA is promising in adjuvant RCC — but current assays are not ready to select patients for or against adjuvant pembrolizumab in routine practice.
In RCC, ctDNA may be prognostic and pharmacodynamic, but “detectable” is not yet the same as “actionable.”
Overall discussion takeaway:
Kidney cancer is clearly moving toward more precision:
➡️ Better disease biology
➡️ Better risk stratification
➡️ Better histology-specific trials
➡️ Better radioligand and bone-directed strategies
➡️ Better biomarkers for adjuvant decision-making
But today’s discussion also reinforces a key principle:
Not every promising signal changes practice immediately.
Some data refine what we should not do yet.
That is just as important for clinical algorithms.
@scocmem@AmandaNizamMD@WeOncologists@montypal@DrDanielHeng@apolo_andrea@DrChoueiri@PGrivasMDPhD@TiansterZhang@neerajaiims@amerseburger@Silke_Gillessen@tompowles1@AndreaNecchi@cdanicas@AOmlin@crisbergerot@HHammersMD@ravikanesvaran@sonpavde@drenriquegrande@scserendipity1@EfstathiouEleni@BraunMDPhD@brian_rini
#KidneyCancer #RCC #nccRCC #ctDNA #GUonc #ASCO26 #OncoAlert
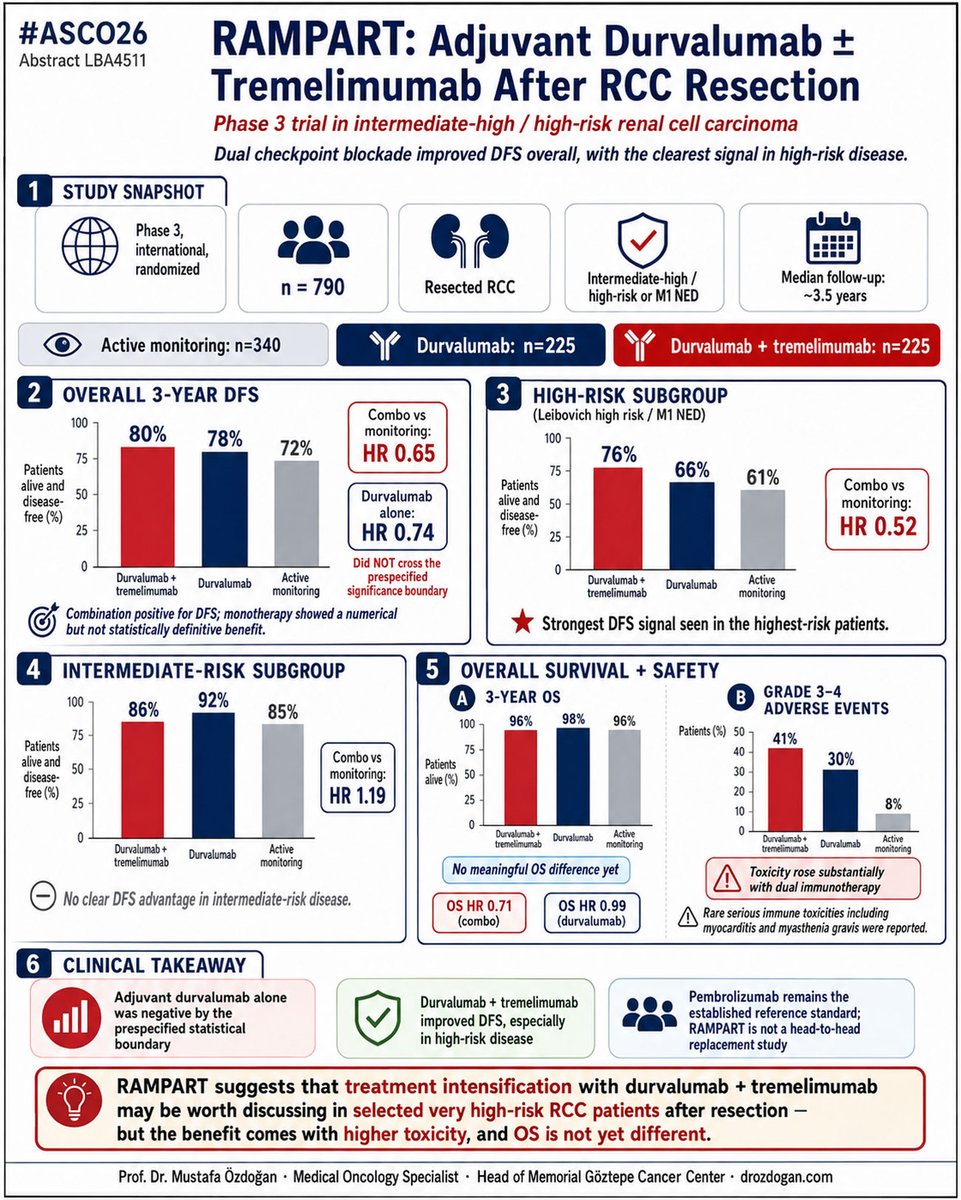
ASCO 2026 | LBA4511 | RAMPART
While dual checkpoint blockade with durvalumab plus tremelimumab demonstrated a DFS benefit in high-risk resected RCC, durvalumab monotherapy did not meet the prespecified threshold for significance. Given the increased toxicity and the absence of a clear overall survival signal, these results do not appear sufficient to displace pembrolizumab from its current position as the established adjuvant standard in this setting.
#ASCO26 #RCC #KidneyCancer
@ASCO@OncoAlert@DrChoueiri@PGrivasMDPhD@montypal@marklewismd@DrYukselUrun@Larvol
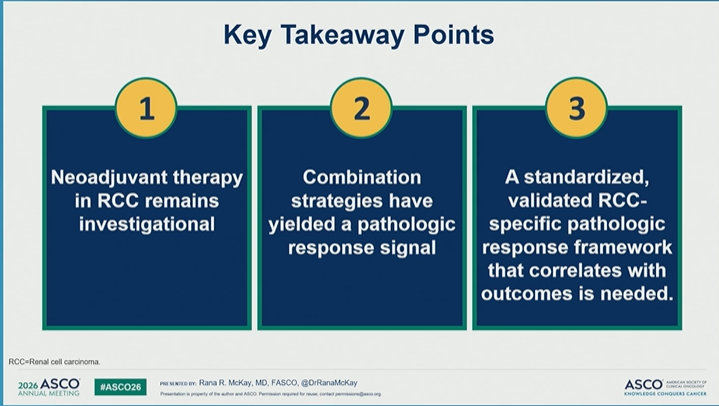
#ASCO26 GU Oncology Spotlight 🚨
🔬 Neoadjuvant Treatment Strategies in Renal Cell Carcinoma
Presented by Rana R. McKay, MD, FASCO
@DrRanaMcKay@OncoAlert@ASCO
Neoadjuvant therapy in RCC remains one of the most important open questions in GU oncology.
The rationale is compelling:
➡️ treat micrometastatic disease earlier
➡️ assess treatment sensitivity in vivo
➡️ potentially downstage tumors
➡️ inform surgical timing
➡️ improve long-term outcomes
But the field is still not ready for routine practice.
Why?
Because activity is not the same as validated clinical benefit.
Modern IO-based regimens can shrink primary kidney lesions in metastatic RCC:
• CheckMate 214: kidney lesion ≥30% decline in 35%
• CheckMate 9ER: ≥30% decline in 51%
• CLEAR: median kidney lesion shrinkage 46%
Pathologic activity has also been reported after IO before nephrectomy:
• 52 patients across 9 sites
• 44% pathologic downgrading
• 13% pCR
These signals are biologically important.
But they do not yet define a standard neoadjuvant approach.
📌 Timing may matter.
In melanoma, trials such as SWOG-S1801 and NADINA support the superiority of neoadjuvant IO over adjuvant-only strategies.
That concept is highly provocative for RCC.
Could immune activation be more effective when the primary tumor is still present?
Maybe — but RCC-specific evidence remains incomplete.
🧪 Current neoadjuvant/perioperative RCC data remain limited.
Several early studies have explored:
• nivolumab
• avelumab + axitinib
• sitravatinib + nivolumab
• nivolumab-based combinations
Most are small phase II or single-arm studies.
And the largest randomized perioperative RCC trial, PROSPER, did not improve EFS:
➡️ nivolumab vs observation
➡️ EFS HR 0.94
➡️ 95% CI 0.74–1.21
So enthusiasm must remain evidence-based.
🧬 The endpoint problem is critical.
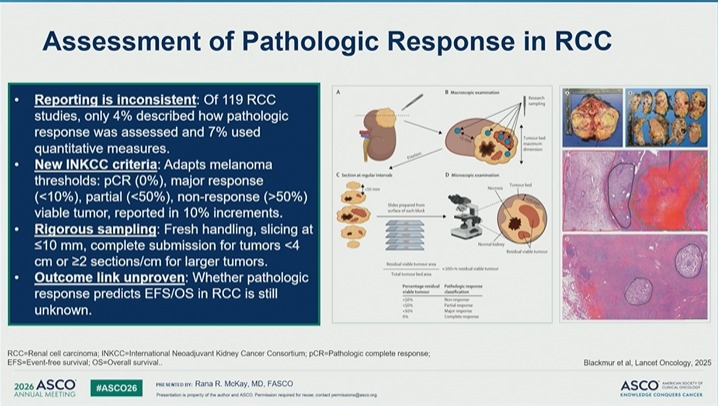
If neoadjuvant RCC is going to move forward, we need standardized pathologic response criteria.
Central principles:
✓ standardized
✓ reproducible
✓ correlated with outcomes
The INMC pathologic response framework categorizes viable tumor in the treated bed as:
• pCR: 0%
• near pCR: ≤10%
• pPR: >10–50%
• pNR: >50%
But reporting has been inconsistent.
In one review of RCC studies:
• only 4% described how pathologic response was assessed
• only 7% used quantitative measures
That is a major limitation.
Unlike some other tumors, we still do not fully know whether pathologic response reliably predicts EFS or OS in RCC.
🚧 New trials are trying to answer the right questions.
NEOSHIFT is testing pembrolizumab + belzutifan before radical nephrectomy in selected clear-cell RCC.
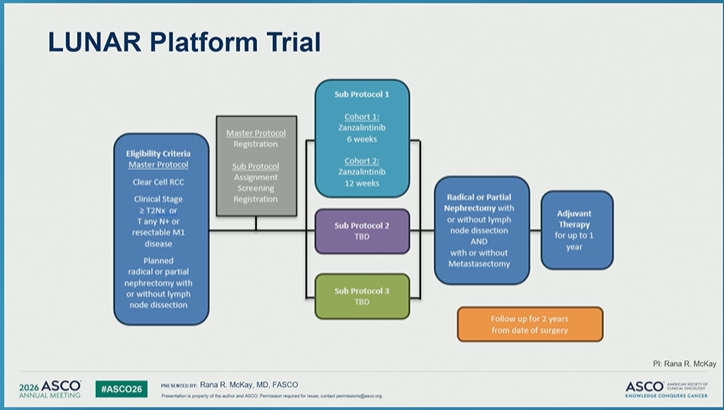
The LUNAR platform is designed to evaluate multiple neoadjuvant strategies in RCC, including systemic therapy followed by nephrectomy and adjuvant therapy.
These platform-style approaches are exactly what the field needs.
💬 My take:
Neoadjuvant RCC is promising — but still investigational.
Combination strategies have generated pathologic response signals.
But before changing practice, we need:
✓ validated RCC-specific pathologic endpoints
✓ biomarkers of response
✓ clarity on surgical safety
✓ correlation with long-term outcomes
✓ randomized evidence
✓ patient selection
The goal is not simply to shrink the kidney tumor.
The goal is to prove that earlier systemic therapy improves meaningful outcomes.
For now, neoadjuvant RCC belongs in clinical trials whenever possible.
@DrChoueiri 🇺🇸@hoperugo 🇺🇸 @matteolambe 🇮🇹 @TiansterZhang 🇺🇸 @CathyEngMD 🇺🇸 @stolaney1 🇺🇸 @montypal 🇺🇸 @tompowles1 🇬🇧 @brian_rini 🇺🇸 @cdanicas 🇪🇸 @NiuSanford 🇺🇸 @amerseburger 🇩🇪 @GlopesMd 🇺🇸 @Icro_Meattini 🇮🇹 @PGrivasMDPhD 🇺🇸 @DrYukselUrun 🇹🇷
#ASCO26 #GUOnc #KidneyCancer #RCC #NeoadjuvantTherapy #Immunotherapy #PrecisionOncology #ClinicalTrials
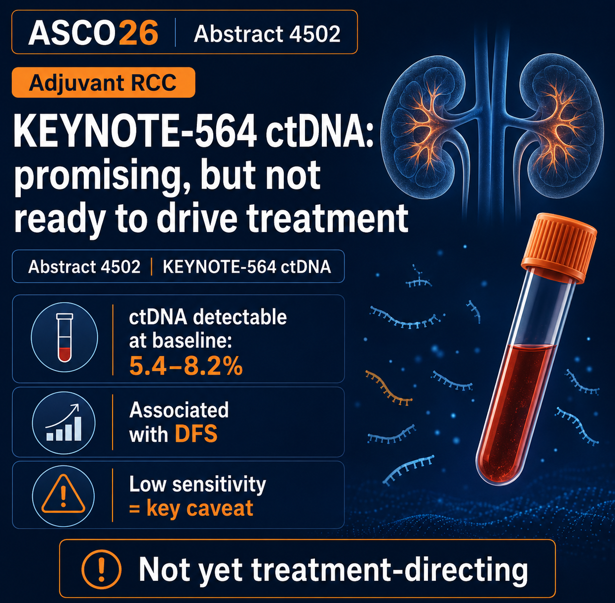
🟠 #ASCO26 GU biomarker highlight | RCC
Abstract 4502 | KEYNOTE-564 ctDNA analysis
Adjuvant pembrolizumab vs placebo in high-risk clear-cell RCC by @DrChoueiri@ASCO@OncoAlert
Clinical question:
Can ctDNA help identify recurrence risk or treatment dynamics in patients receiving adjuvant pembrolizumab after nephrectomy for high-risk ccRCC?
Main finding:
Baseline ctDNA positivity was uncommon:
5.4% with the 16-plex assay
8.2% with the 64-plex assay
ctDNA positivity was negatively associated with DFS, and ctDNA change from baseline to cycle 5 day 1 was associated with DFS in both treatment arms.
Why it matters:
We urgently need better tools in adjuvant RCC to identify who is at highest risk, who benefits most, and who may be overtreated.
Important caveat:
The low detection rate matters. Baseline ctDNA had low sensitivity but high specificity for DFS prediction. This is not yet a treatment-selection tool for routine adjuvant RCC decision-making.
My take:
The biology is compelling, but RCC remains a difficult ctDNA disease. These data support continued MRD research, not ctDNA-driven withholding or escalation of adjuvant pembrolizumab today.
#KidneyCancer #RCC #ctDNA #GUonc #ASCO26
@DrRanaMcKay@ALLIANCE_org PhII RADICAL adv #RCC (majority pretreated w/1 bone met) of cabo +/- Ra-223 ➡️ n=98 due to #SSEs in combo leading to early closure but numeric ⬆️ in OS 28.3 vs 19.7 mos w/late separation in favor of combo but not significantly diff #ASCO26@OncoAlert
#ASCO26 KEYNOTE-564 🧬ctDNA analysis: ctDNA positivity was prognostic, but sensitivity was low.
Useful biology, but not all assays are ready for clinical decision-making.
❓Would you act on ctDNA in adjuvant RCC today?
@DrChoueiri@DrYukselUrun@OncoAlert@NazliDizman #KidneyCancer #GUonc #oncology @ONCOassist@AUC3_Official
Clear cell RCC sheds low levels of ctDNA, but positivity and ctDNA dynamics are relevant in the adjuvant setting @DrChoueiri#ASCO26. This analysis is with an exome based personalised technique and shows a lack of sensitivity (5-8% ctDNA+ve rate vs 40% radiological relapse rate) but good specificity (almost all ctDNA +ves relapse). Whole genome ctDNA analysis should work work better. There is a future for ctDNA in renal cancer, we’re just not quite there yet IMO.
“Is the Best Yet to Come in Kidney Cancer?” Detailed and well framed discussion by @MVossMD on the 3 RCC studies: bone mets, non-clear cell RCC, and ctDNA in adjuvant KEYNOTE-564.
#ASCO26#RCC@OncoAlert@ASCO@OncBrothers
Important survivorship perspective in RCC presented by #ElizabethNally: decision regret after adjuvant pembrolizumab was driven more by chronic low-grade/life-changing toxicity than by recurrence itself, highlighting limitations of CTCAE alone.
#ASCO26#RCC@OncoAlert@ASCO@OncBrothers
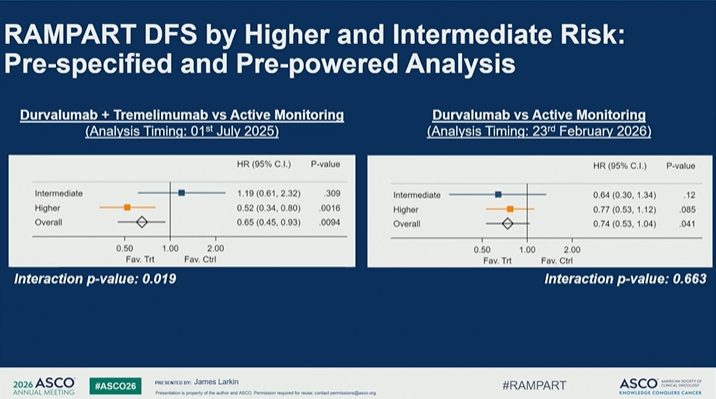
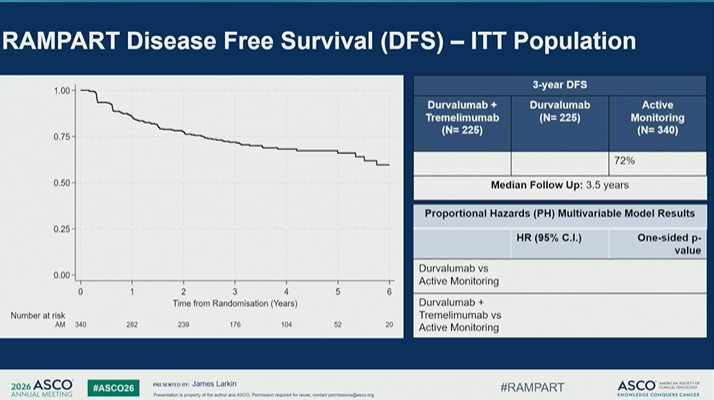
🔬 LBA4511 | RAMPART
Adjuvant durvalumab ± tremelimumab vs active monitoring after resection of RCC
Presented by James M.G. Larkin, MD, PhD
@OncoAlert@ASCO
Adjuvant therapy in RCC remains one of the most nuanced areas in GU oncology.
We have a clear positive story with pembrolizumab from KEYNOTE-564, but other adjuvant immunotherapy strategies have shown mixed or negative results.
RAMPART adds an important new piece to this puzzle.
🧪 Study design
Patients had resected RCC with:
• high or intermediate risk of relapse by Leibovich score
• or fully resected synchronous ipsilateral adrenal metastases
• or a single fully resected soft tissue metastasis
Randomization:
• durvalumab + tremelimumab
• durvalumab alone
• active monitoring
Primary endpoint: disease-free survival
The analysis included a prespecified, pre-powered evaluation by baseline relapse risk.
📊 Key DFS signal
In the overall analysis:
➡️ Durvalumab + tremelimumab vs active monitoring
HR 0.65
p = 0.0004
➡️ Durvalumab vs active monitoring
HR 0.74
p = 0.041
But the clinically important story is the risk subgroup.
📌 Higher-risk subgroup
3-year DFS:
• Durvalumab + tremelimumab: 76%
• Durvalumab: 66%
• Active monitoring: 61%
For higher-risk disease:
➡️ Durvalumab + tremelimumab vs active monitoring
HR 0.52
p = 0.0016
➡️ Durvalumab vs active monitoring
HR 0.77
p = 0.085
So the clearest signal appears to be with dual checkpoint blockade in higher-risk RCC.
⚠️ Why this matters
RAMPART suggests that adjuvant CTLA-4 + PD-L1 inhibition may reduce recurrence risk in selected higher-risk patients after RCC resection.
But this is not a simple “treat everyone” message.
Important caveats:
🔹 Benefit appears risk-dependent
🔹 Durvalumab monotherapy looks less convincing
🔹 OS data are still needed
🔹 Toxicity and long-term immune effects matter in the adjuvant setting
🔹 Treatment completion was limited
Treatment exposure reminds us how hard adjuvant immunotherapy can be:
• Durva+trem completed per protocol: 23%
• Durva alone completed per protocol: 32%
• Median treatment duration: ~11 months
💬 My take
RAMPART strengthens the idea that adjuvant therapy in RCC should become more risk-adapted.
The signal with durvalumab + tremelimumab in higher-risk RCC is clinically interesting and potentially important.
But in the adjuvant setting, the bar is high.
We need to balance:
✓ recurrence reduction
✓ OS maturity
✓ immune toxicity
✓ patient selection
✓ treatment completion
✓ patient preference
The next step is not simply “more immunotherapy after nephrectomy.”
It is better selection of who truly needs escalation — and who can safely avoid it.
#ASCO26 #GUOnc #KidneyCancer #RCC #Immunotherapy #AdjuvantTherapy #PrecisionOncology
@crisbergerot@HHammersMD@ravikanesvaran@sonpavde@drenriquegrande@scserendipity1@EfstathiouEleni@BraunMDPhD@brian_rini
Congratulations to @BethN01 on a stellar presentation at #ASCO26!
A fascinating discussion on decision regret & toxicity perception following adjuvant ICI therapy in RCC
Thank you to @BethN01 and @tompowles1 for including me in this meaningful work