🇨🇳 A new report from a military medical center in Beijing demonstrates a benefit with daily (QDay) lung SBRT schedules, particularly for stage I NSCLC tumors with high SUV values. Full disclosure: I can't remember the last time I prescribed lung SBRT as QOD. https://t.co/7WbZSkku9V
Radiotherapy Review in NEJM:
“Underuse and refusal of indicated radiotherapy have been shown to increase cancer-specific mortality and the risk of death in both curative and palliative settings”
https://t.co/AVKnIbrw6M
New in Advances in Radiation Oncology:
Wallach et al. propose “curative oligometastatic radiotherapy” (CORT) as a distinct treatment-intent category for carefully selected patients with oligometastatic disease when cure, or exceptionally durable disease control, may be attainable.
The concept goes beyond metastasis-directed therapy alone: all known disease, including the primary when needed, is addressed with curative intent.
Proposed favorable features include limited metastatic burden, favorable disease biology or effective systemic options, controlled extracranial disease, good performance status, low tumor markers or favorable ctDNA, and a long disease-free interval.
The nuance: this is a terminology and clinical framework, not a validated prognostic model. CORT may improve communication, shared decision-making, trial design, and data collection, but selection must remain individualized and disease-specific.
A useful reminder that metastatic disease does not automatically make every course of radiotherapy palliative.
#radonc #OligometastaticDisease #OncTwitter
🚨CAN-2409 + RT: not just delaying PSA failure, reducing residual tumor in the gland.🚨
@TheLancetOncol
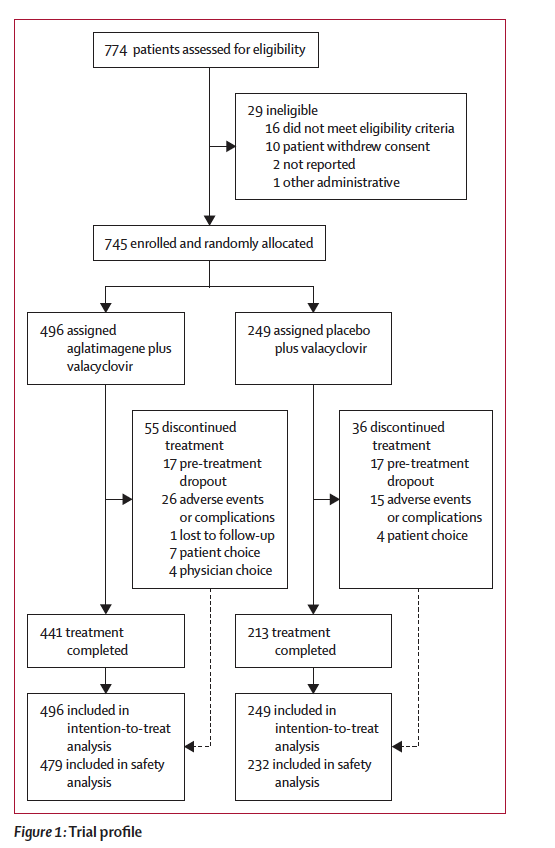
👉Phase 3, double-blind RCT
🧑🤝🧑745 pts w/ int/high-risk localized #prostatecancer
⚖️EBRT + intraprostatic CAN-2409/valacyclovir vs placebo.
💉CAN-2409 is a replication-defective adenoviral HSV-tk gene therapy injected into the prostate.
💊Valacyclovir acts as the prodrug to drive local tumor-cell kill + immune priming
📉 DFS improved: HR 0.70; median NR vs 86.1 mo.
🔬 Key nuance: DFS included local failure by centrally reviewed positive prostate biopsy, protocol biopsy ~2 yrs post-EBRT.
🎯 At 22–26 mo: positive biopsies 20% vs 36%; pCR 80% vs 63%.
🛡️ No major toxicity penalty: grade ≥3 TEAEs 8% vs 7%; no treatment-related deaths.
🔑CAN-2409 may not just suppress biochemical recurrence, it may deepen local tumor eradication after RT.
@PCFnews@PCF_Science@urotoday@UrologyTimes
🔗https://t.co/GyvKotnfdK
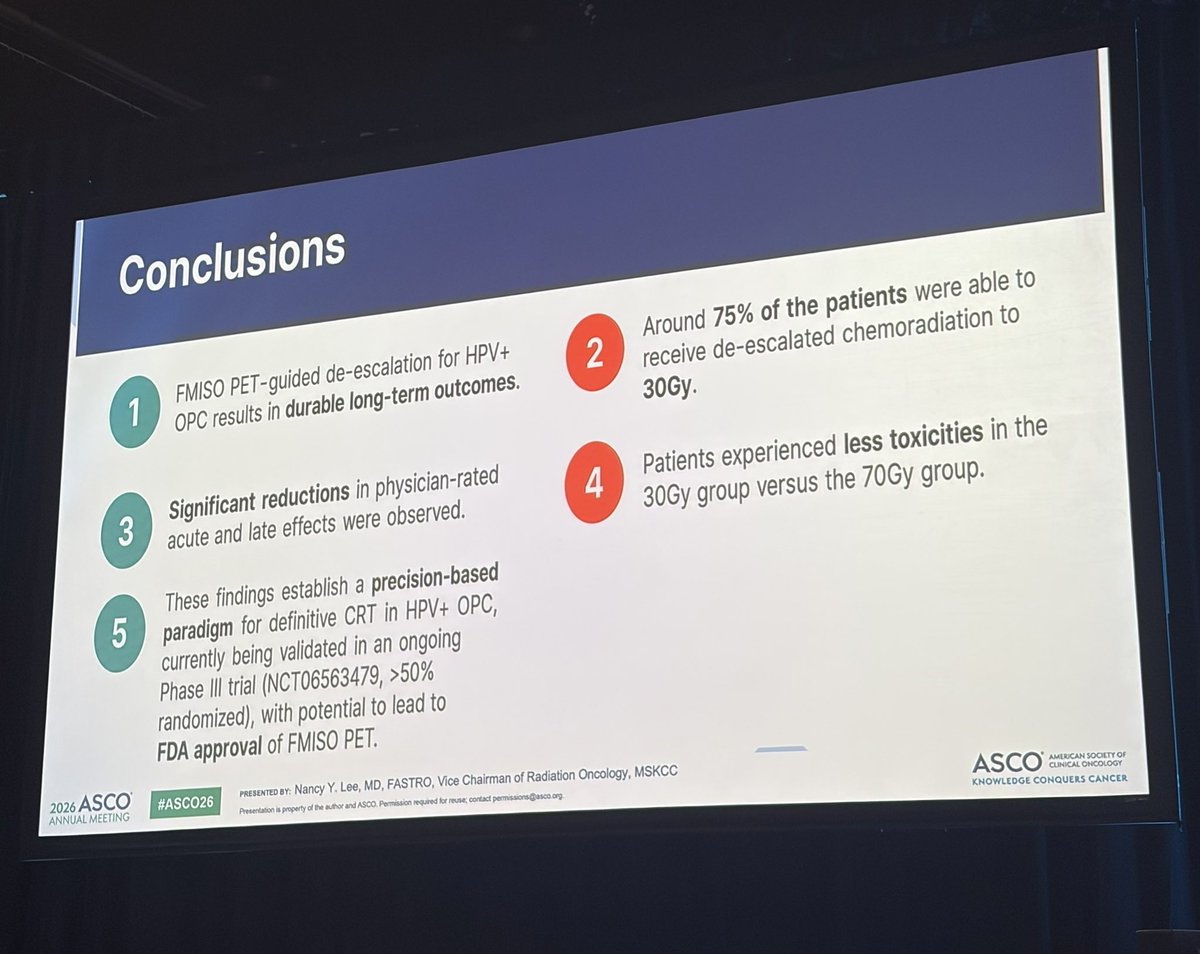
Today at #ASCO26: MSK radiation oncologist Dr. Nancy Lee (@imrtlee) shared long-term results showing that many patients with HPV-positive #oropharyngeal cancer were able to receive lower-dose radiation while maintaining durable outcomes and experiencing fewer side effects.
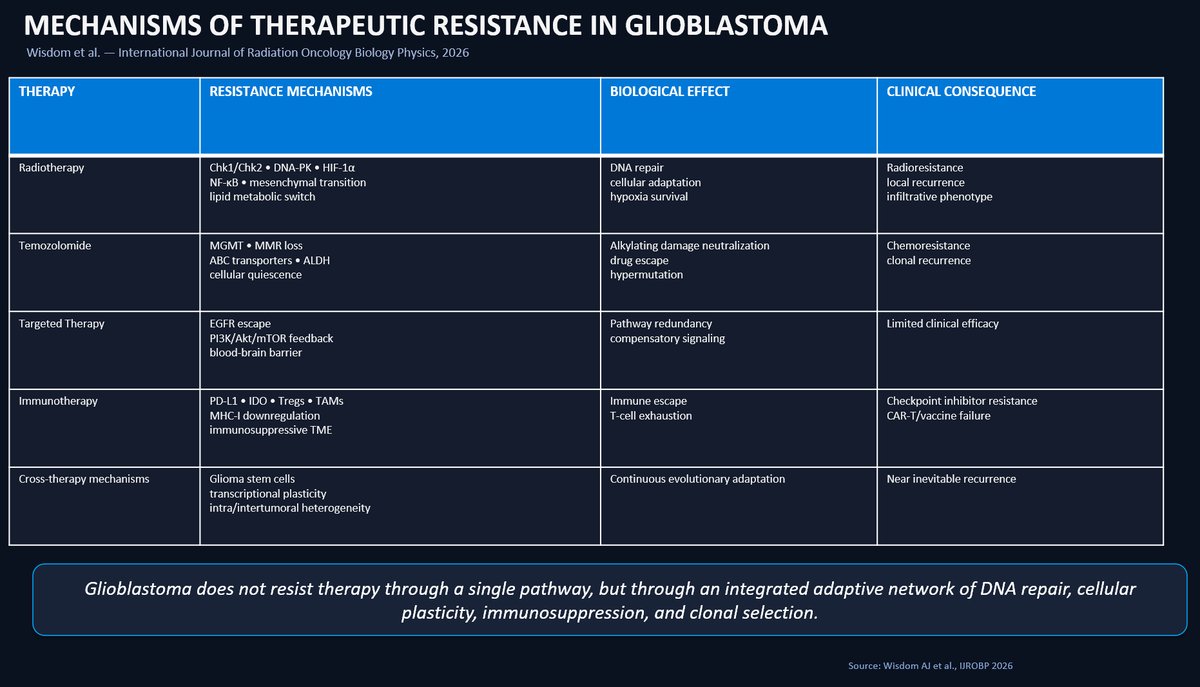
Very deep review in press in @IJROBP about mechanism of resistance in #Glioblastoma (@AmyWisdom8 et. al DOI :https://t.co/fXQmnhMI3R) .This table provides an at-a-glance overview of the main resistance mechanisms discussed in the paper. #radonc
Day 5 of the #ESTRO26#SFRT journey:
☢️ Last but not least, “The potential synergy between SFRT and #immunotherapy” by Slavisa Tubin, Chair of the ESTRO SFRT Focus Group
💻 More activities from the SFRT Focus Group are upcoming: https://t.co/nrg1pcuCMu
@ESTRO_RT@OncoAlert
❗️ The OLIGOMA trial results just dropped at #ESTRO26 and they are massive. A 15-month improvement in median PFS for OMD breast cancer (HR = 0.48). This adds to the growing mountain of evidence that MDT (Metastasis-Directed Therapy) works. Lets’s go 🧵 1/n
More than a review: a mini-treatise on spinal oncology.
Two crucial lessons for #radonc:
• SBRT patient selection must be driven by SINS stability criteria;
• the thecal sac may represent a “natural PRV” for spinal cord constraints.
Outstanding clinical insights !
Honor to give Radiation Oncology National Grand Rounds for @DeptVetAffairs. These radoncs are dedicated to caring for veterans and provide the best care possible. I was humbled to provide insights on re-irradiation with spine #SBRT. Thank you Dr. Jonathan Wallach for organizing.
🧵 Just published in @TheLancet: TORPEdO – the first phase 3 RCT designed specifically to test whether IMPT (proton beam) improves late function & QoL vs modern IMRT in oropharyngeal SCC.
Short answer: It doesn’t.
Long answer (with the numbers that matter) 👇
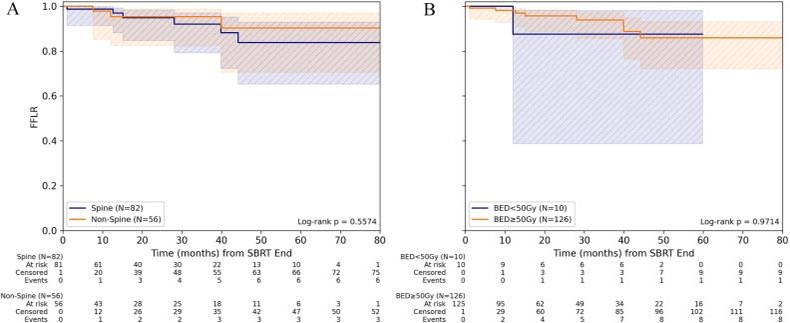
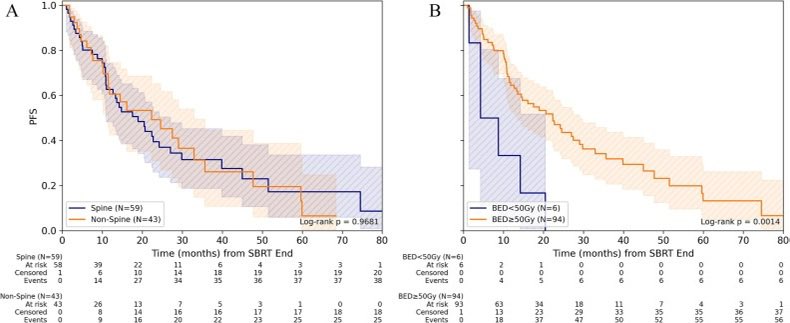
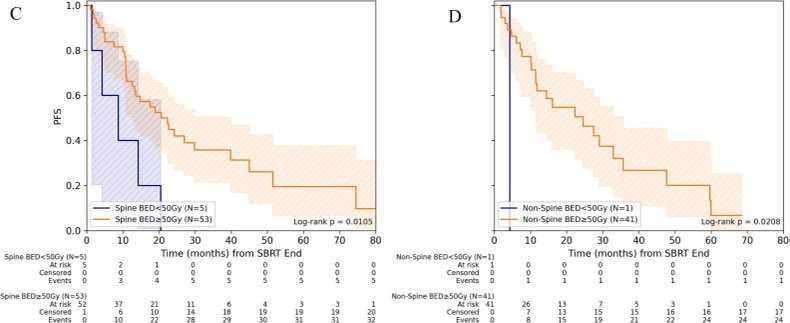
📌 Stereotactic body radiotherapy in patients with bone oligometastases from breast cancer – results from a European multicenter cohort study ☢️🌍
🔗 https://t.co/pwuoGoNe1D
@OncoAlert#OncoAlertAF#BreastCancer#RadOnc
🔹Stereotactic radiotherapy of bone oligometastases with excellent local control. 🔸Well-tolerated treatment with especially low fracture rates. 🔹Prospective studies are needed to determine the role of standardized SBRT concepts.
@DrSpratticus@CShahMD@ASRT@ASTRO_org Great points and ones that bring into question why you would want to train others to do something that will quickly be automated, just for short term convenience.
What will you have them do when it becomes automated?
If it’s more of our tasks, are we overtraining physicians?
Grateful to @ASTRO_org for releasing a statement highlighting their lack of support for the concept of APRTs in the United States. It’s not what’s best for patients most importantly or the specialty. @NehaVapiwala@SameerKeoleMD
https://t.co/fCS5bBQCst
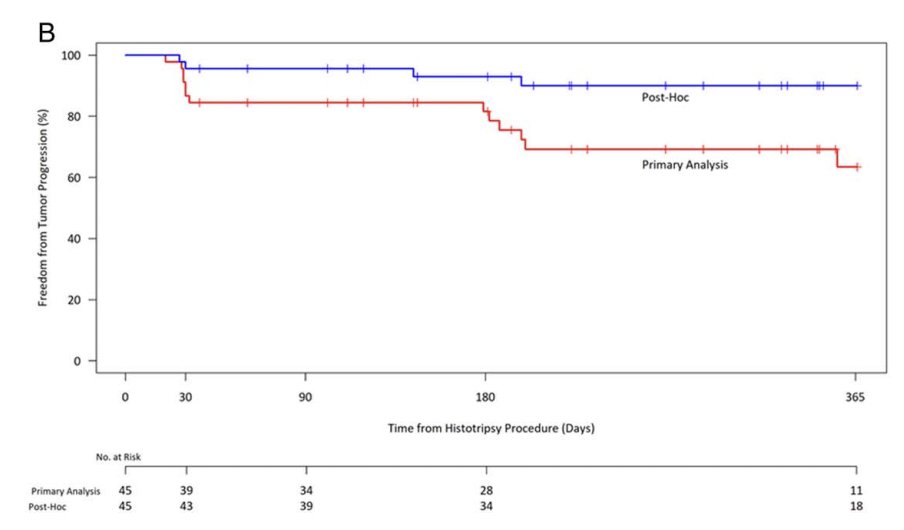
Wow, many issues w this 47-pt, sponsor-run, single-arm histotripsy study.
Short 🧵 1/4
1. Post-hoc imaging re-read: primary read w validated criteria showed 1-yr LC 63%, but they emphasize a post-hoc re-read (using new “experience” w histo imaging) bumping local control to 90%.