#EuroPCR
💥 LM Perforation : a rare but catastrophic complication
Prevention Is Better ❗️
But When It Happens :
🚨Recognise it immediately
🚨The team must be there
🚨Remember to have covered stents in the lab
A backtable illustration of a couple techniques you can use if the #Rotaburr gets stuck,
1-The skipping rope technique.
We have known it for a couple years, and it was recently published
https://t.co/fqTn6NXkaT
2-The final resort of cutting the rota driveshaft and advance a guideliner through it to get more leverage to pull.
Of course the first thing you do is to pull hard and maybe try to balloon around it, but those can help with tougher situations.
#CardioX community, please share your additional tips and comments
𝟭/𝟴 🚨 Big news in cardiology!
The 𝗟𝗘𝗖𝗔𝗥𝗧 𝗧𝗿𝗶𝗮𝗹 just dropped at EHRA 2026.
Left Bundle Branch Area Pacing (𝗟𝗕𝗕𝗔𝗣) takes on Biventricular Pacing (𝗕𝗶𝗩𝗣) to see which is superior for Cardiac Resynchronization Therapy (CRT).
Let's dive into the results of this late-breaking trial! 🧵👇
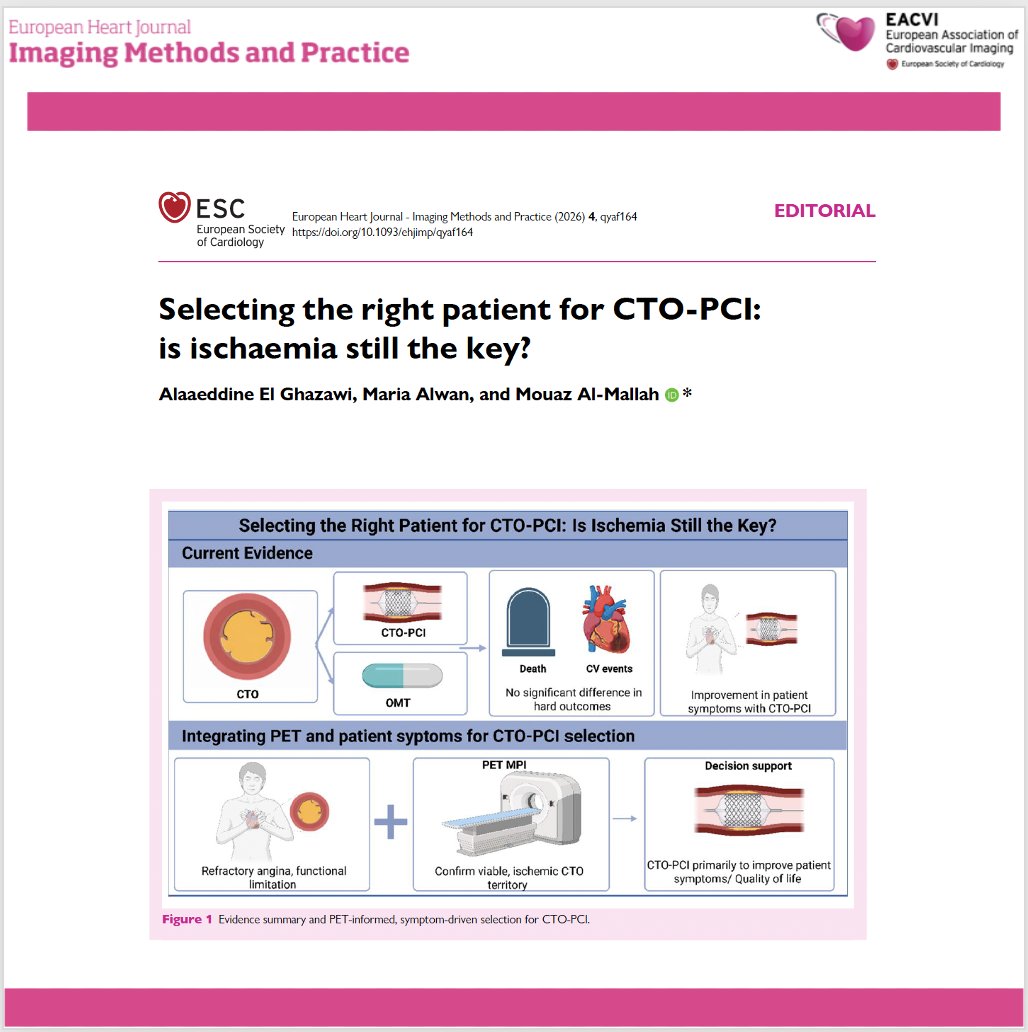
📄 CTO-PCI: is ischaemia still the key for patient selection?
🔗 DOI: https://t.co/1OtXRpQLiq
🫀 Chronic total occlusion (CTO) PCI has evolved significantly, with high success rates—but patient selection remains the real challenge.
This editorial questions a long-standing paradigm:
👉 Is ischaemia enough to guide revascularization?
✨ Key insights:
🔹 CTO-PCI is associated with:
✔ improved symptoms and quality of life
❗ but no clear reduction in mortality or major events
🔹 Randomized trials show:
➡️ similar hard outcomes vs optimal medical therapy
➡️ benefit mainly in angina relief
📊 Role of ischaemia:
👉 Imaging confirms ischaemia—but:
❗ baseline ischaemic burden does NOT predict outcomes after CTO-PCI
🔹 Even patients with ≥10% ischaemia:
➡️ no difference in mortality or MACCE
➡️ but fewer angina hospitalisations
⚠️ Why ischaemia alone is insufficient:
👉 CTO physiology is complex:
collateral circulation
multivessel disease
microvascular dysfunction
👉 SPECT may underestimate disease
👉 PET provides better quantification (MBF, MFR)
💡 Clinical paradigm shift:
👉 From “ischaemia-driven” → “symptom-driven” selection
✔ Revascularize when:
refractory angina
significant functional limitation
👉 Imaging role:
➡️ confirm viable, ischaemic myocardium
➡️ support—not dictate—the decision
🧠 Future directions:
🔹 PET-based quantification (MBF/MFR)
🔹 Territory-specific ischaemia assessment
🔹 Integration of patient-reported outcomes
🚨 Bottom line:
CTO-PCI is a tool to improve symptoms—not to change prognosis.
👉 Treat the patient, not just the ischaemia.
#Cardiology #CTO #PCI #Ischaemia #CardiacImaging #PET #CoronaryArteryDisease #InterventionalCardiology #PrecisionMedicine 🫀📊
Summary of all Late-Breaking Trials at #ACC2026 – take home points
@ACCinTouch@ACCmediacenter@JACCJournals
1. HI-PEITHO: Ultrasound-facilitated catheter-directed thrombolysis led to a lower risk of PE-related death, cardiopulmonary decompensation or collapse, or recurrence of PE. vs anticoagulation alone in intermediate-high risk PE.
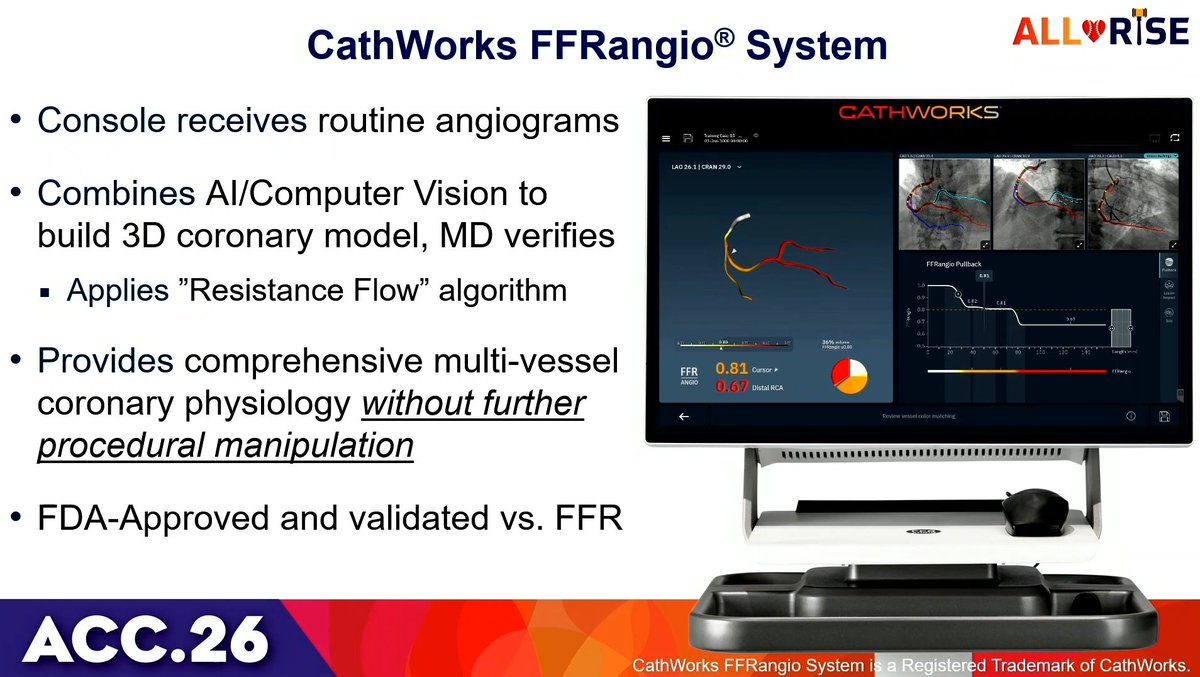
OPTIMAL suggests that using IVUS in unprotected left main PCI may cost you 22 minutes with no clinical benefit. One might think it’s an outlier. Yet, the same day, IVUS-CHIP reports no advantage of IVUS over angiography in complex high-risk PCI. Either we have been fundamentally misinterpreting the evidence so far, or we urgently need to reconcile these data. #ACC26
https://t.co/eoJzCtVy8h
https://t.co/6kYUhV1Sbm
Aptly named ALL RISE trial at #ACC26. Wire based FFR vs conventional Angiogram based FFR. Despite large data Physiological assessment in lab still low for well known reasons. With non-inferiority of trial, probably it's time to quickly adopt the angiogram based FFR and move away from percent stenosis that leads to occulo-stenotic PCI. Hopefully implementation is not expensive.
1/16 🧵 ORBITA-CTO: The first randomized, placebo-controlled trial of CTO PCI.
📰 Published in JACC, presented at #ACC26.
🔬 Finally, sham-controlled evidence for what we do in the cath lab every day.
One of the best designed studies I have ever seen!
A biostatistical deep dive. Let's go. 👇
HI-PEITHO key takeaways #ACC26
🫀 Intermediate-risk PE = stable patients with RV strain + positive biomarkers
⚖️ ultrasound-facilitated catheter-directed thrombolysis + AC vs AC alone in this “gray-zone” group
📉 ↓ Early clinical deterioration: 4.0% vs 10.3%
🚑 Benefit driven by ↓ hemodynamic collapse—not mortality
🩸 No ↑ major bleeding or ICH → supports selective early intervention
Early Surgery or Conservative Care for Asymptomatic Aortic Stenosis at 10 Years: @NEJM
🥸 Asymptomatic severe AS - more evidence accumulate
😱 Let's summarize the RECOVERY trial
👇👇👇👇
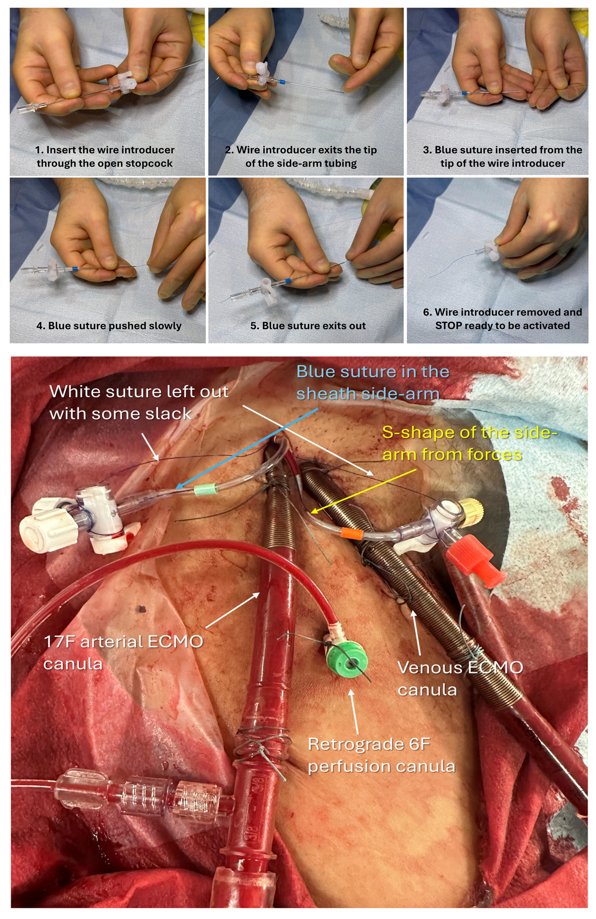
Welcome to the Side-Arm Technique on Perclose (STOP) technique: a simple, low-cost method to prevent or stop bleeding from large bore indwelling catheters by activating Perclose sutures for complete entry site sealing https://t.co/22fym9NMY9 @ccijournal
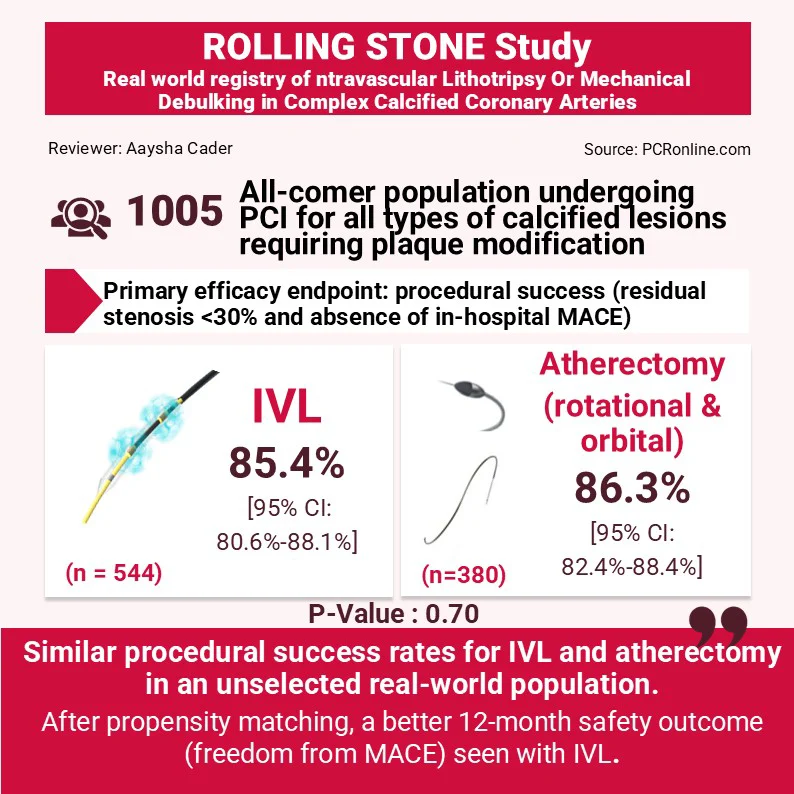
ROLLING STONE: Intravascular lithotripsy or mechanical debulking in complex calcified coronary arteries
🔗https://t.co/TZRvWgwOKf
Journal Club: @aayshacader reviews ✍️this multicenter, prospective study 📊 that compares IVL and atherectomy (rotational and orbital) for treating heavily calcified coronary arteries, assessing real-world safety and effectiveness in PCI.
#clinicaltrial #science #interventionalcardiology #cardioX
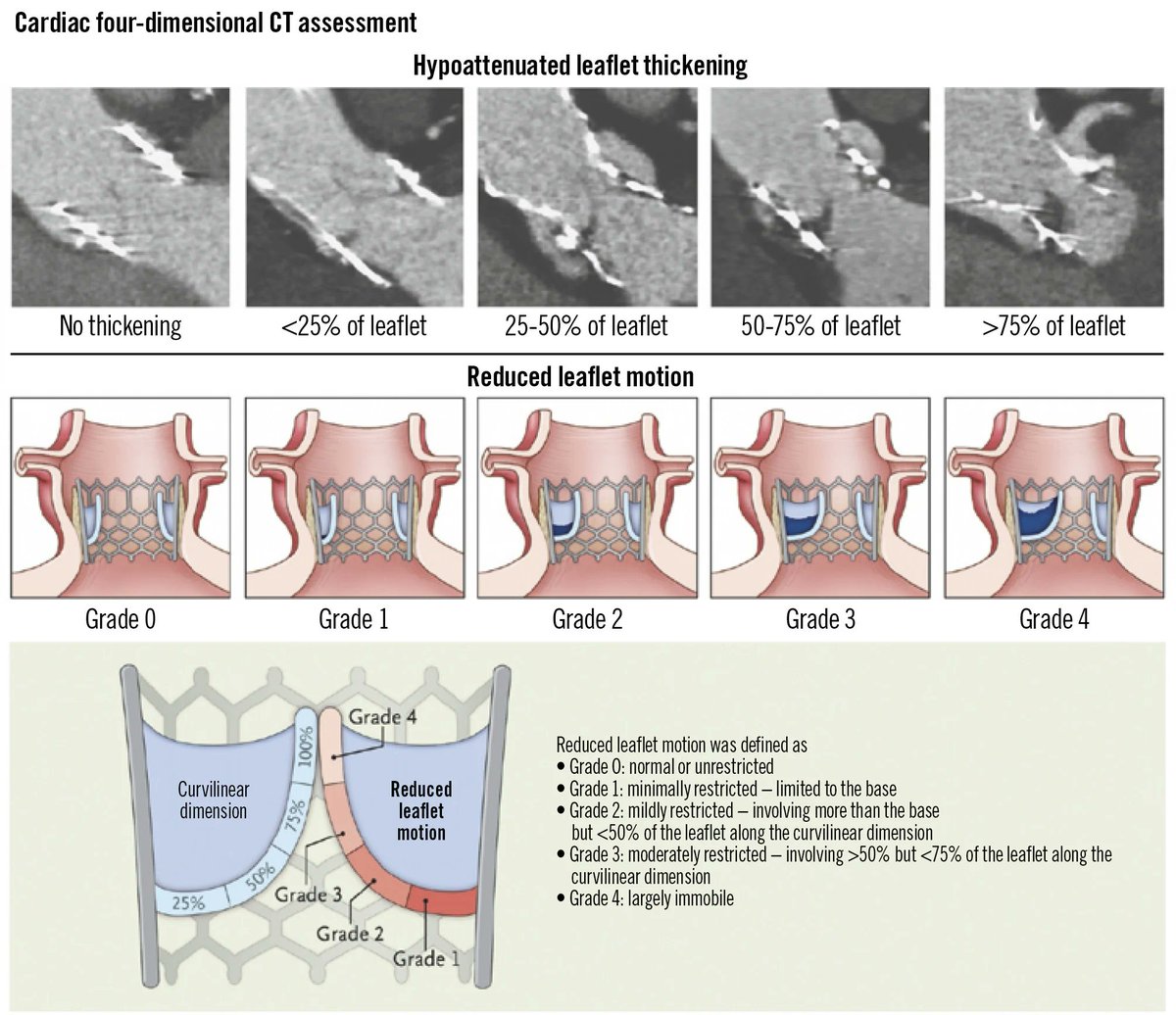
This state-of-the-art review outlines current evidence on the mechanisms, prevalence, clinical relevance, and management of TAVI thrombosis and highlights ongoing clinical trials investigating this condition. https://t.co/zmRnf6hjZo