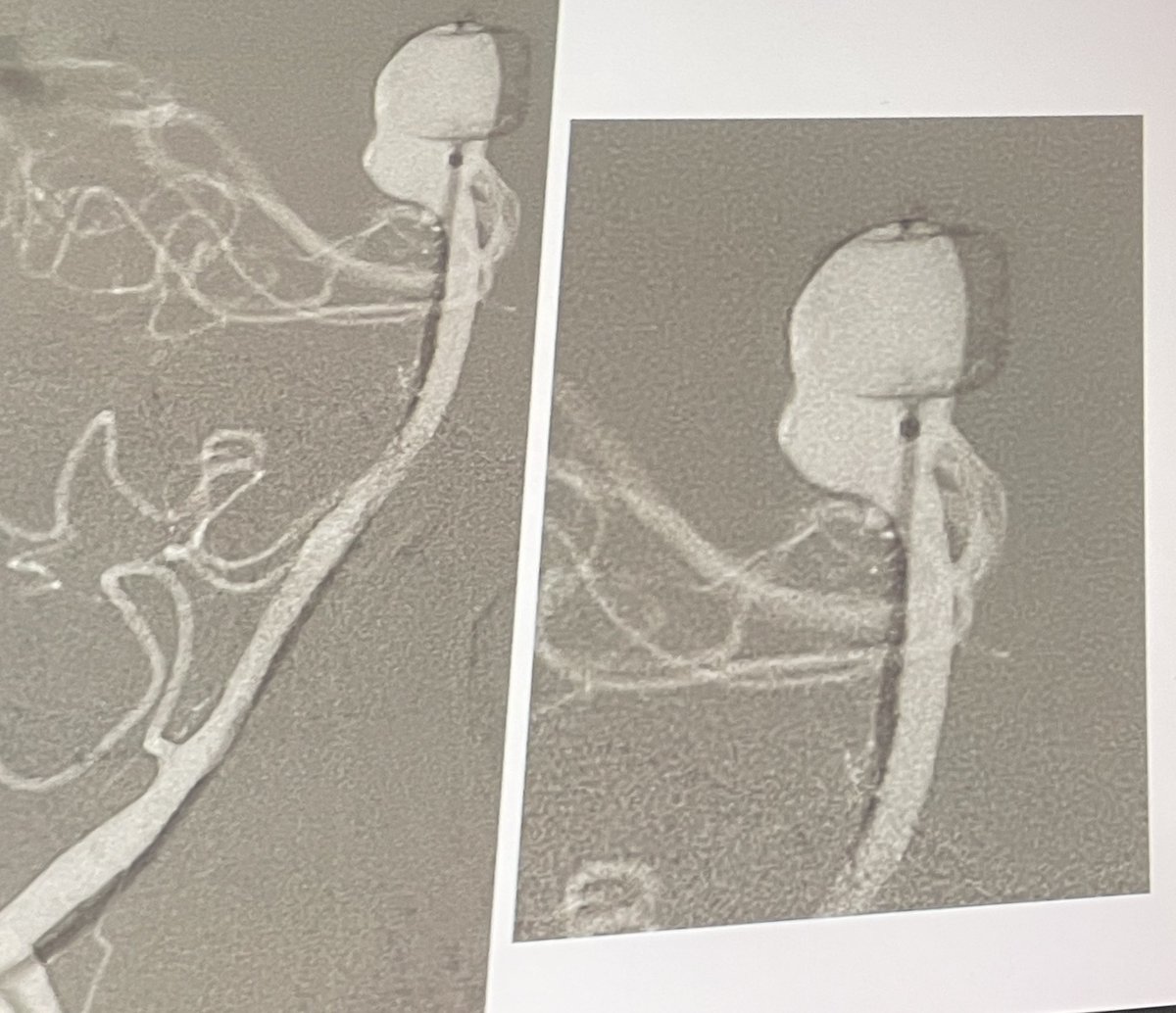
Foramen magnum-marginal sinus dural arteriovenous fistula presenting with brain stem edema and progressive myelopathy.
Skull base and cerebrovascular surgery-the inseparable twins (citing @jacquesmorcosmd). Far lateral approach provided the exposure needed for precise microsurgical disconnection of the fistula resulting in symptoms resolution. @MariaBederson@StanfordNsurg
The literature has consistently supported that a retro odontoid pannus will regress over time with atlantoaxial fixation and fusion. On rare occasion, compressive cysts can accompany the pannus, leading to progressive myelopathy. The literature is not as clear in this setting regarding the timing of cyst regression after fusion. There are times when it is necessary to think outside the box in order to rapidly get the patient’s cord out of trouble, providing a direct & immediate decompression.
In this surgical video and manuscipt, we detail our posterior transdural approach for resecting a retro-odontoid cyst causing neurological decline.
Many thanks to Mark Shornak for his complementary illustrations.
https://t.co/egcJhB1UJq
@TheJNS@AANSNeuro@spinesection@uncneuro@unc_neurorads@UNCneurosurgery
In 1980, DeBakey operated on the Shah of Iran. He declares success. Soon, the patient is dead. Reoperation is psychologically brutal: how bias delay truth & what might save us from the same trap. https://t.co/5nZdjJEcmA #MedTwitter#Surgery#MedEd
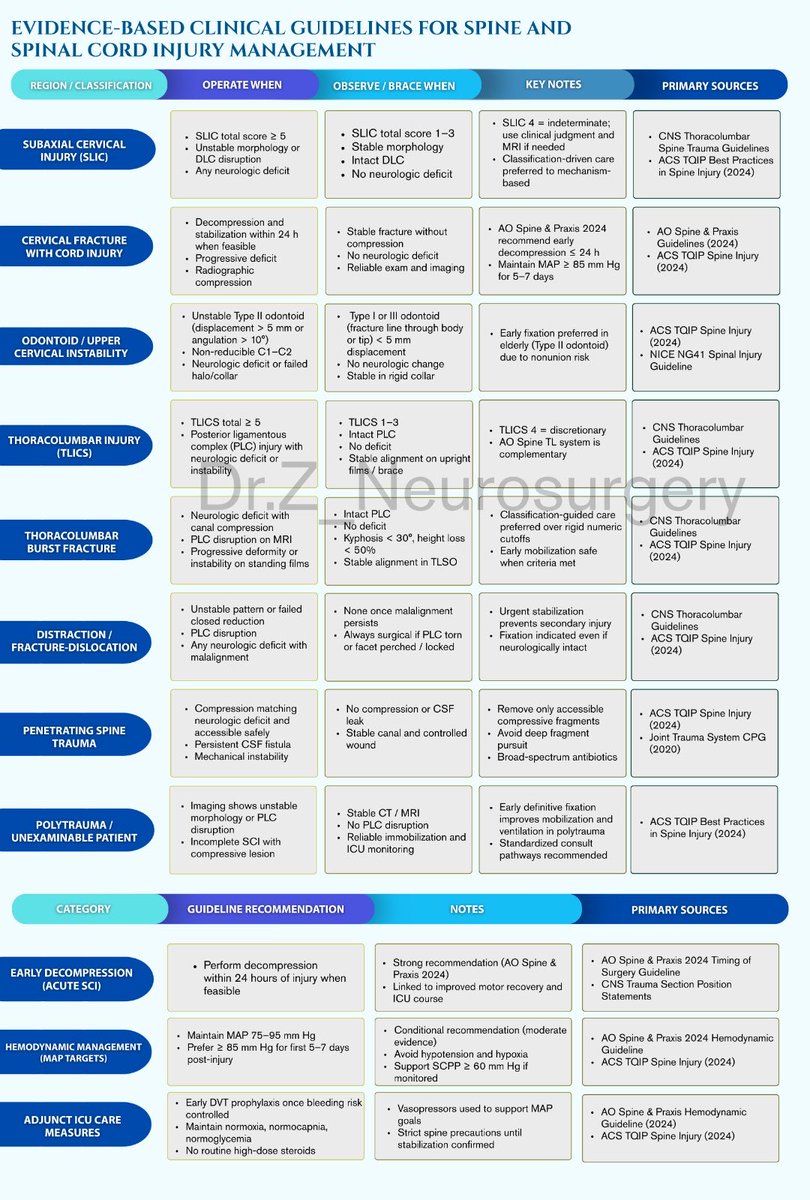
I compiled this flow chart based on the most recent clinical guidelines for spinal trauma. It includes when to operate immediately, when it’s OK to observe, and some important ICU-level management regarding perfusion pressure and arterial pressure.
Clinical guidelines are very important for us to be able to have a uniform understanding of what’s considered a surgical emergency versus something that can be monitored. As of right now this is what the most recent data tells us.
Recently tried the 7Fr radial balloon guide PATH catheter by Crossroads Neurovascular and encountered a radial loop. Radial loops are present in 1-2% of the population. They can be reduced, though often it is painful in the awake patient.
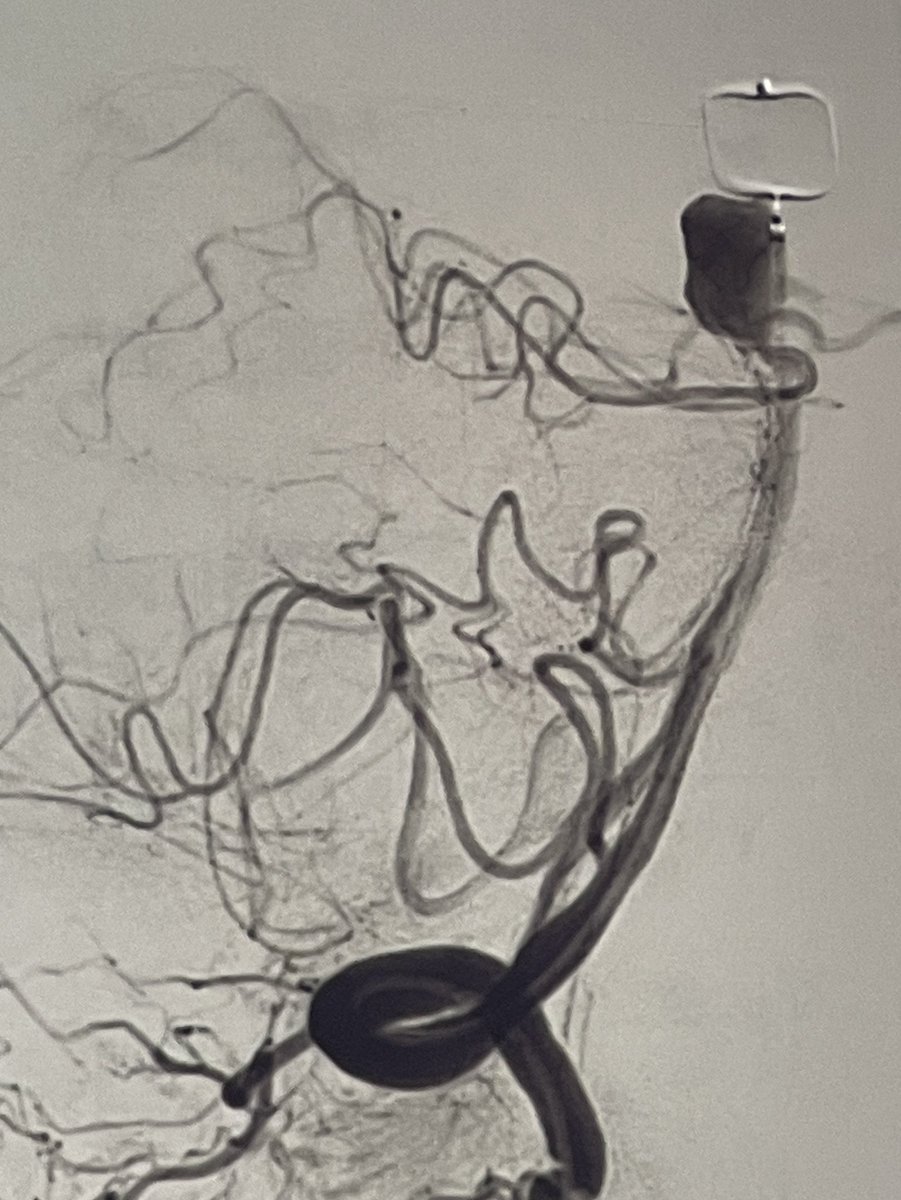
SAH case with no aneurysm. The key? Not a positive finding - a negative one. After proper angling & longer injection, proximal PICA showed up. Distal portion occluded from dissection. Treated with PAO. Patient did well with partial Wallenberg. Always look for what's not there.
Diagnosing/localizing CSF leak is harder than treating. But transdural repair for ventral bone spur is beautiful, technical surgery
March 2025 @StrokeBern series showed no diff bw suture and patch, though I like both
@NeurosurgeryCNS PMID 39132996 @WouterSchievink@tdobrocky
One of the hardest tumors I’ve tackled in a long time. 2 year-old male presents with vision loss and sleepiness. Biopsy shows adamantinomatous craniopharyngioma. Subfrontal approach. Encasing every major neurovascular structure of the skull base. Was able to take it back to the hypothalamus, the chiasm, and dissect off the nerves and vessels. Likely stage 2 transcallosal from the top needed. Thinking about toci/avastin. Thoughts? @PhxChildrens@BarrowNeuro