‼️⚠️Please read this until the end.
A widely shared article has presented a deeply misleading view of Long COVID, suggesting once again that cognitive behavioral therapy, exercise, and “mind-body” approaches may be the uncomfortable truth patients refuse to accept.
This needs to be challenged.
Not because the nervous system does not matter.
Not because psychological support cannot help.
But because confusing support with cure, physiology with psychology, and heterogeneity with “it might be in your head” is exactly how medicine has harmed post-infectious patients for decades.
There are articles about Long COVID that look like science journalism, but in reality they repackage, in modern language, a very old idea: if we do not fully understand a disease, maybe the problem is in the patient’s mind.
And that is not science. That is repeating history.
The article begins with a striking sentence:
“There isn’t a single approved pharmaceutical treatment, not even a test to verify the presence of the illness.”
This may sound forceful, but it is a very misleading way of presenting the problem.
The fact that there is still no drug specifically approved for Long COVID, or a single diagnostic test, does not mean that “nothing has been found.” It means that we are dealing with a heterogeneous disease, probably with several biological subgroups, and that medicine has not yet converted those findings into validated clinical tools.
“No single diagnostic biomarker” is not the same as “no biology.”
In just a few years, immunological, vascular, neurological, endocrine, and metabolic abnormalities have been described in subgroups of Long COVID patients: autonomic dysfunction, herpesvirus reactivations such as EBV/HHV-6, alterations in the cortisol axis, autoantibodies against GPCR receptors — including adrenergic and muscarinic receptors — persistent viral antigens, endothelial damage, muscle abnormalities after exertion, mitochondrial dysfunction, persistent inflammation, and differential immune changes.
Is everything settled? No.
Does that mean it is psychological? Also no.
Science does not work like that. Multiple sclerosis did not stop existing before we had MRI. Many autoimmune diseases do not show up in routine blood tests. If a complete blood count, a basic biochemistry panel, or an X-ray comes back “normal, normal, normal,” that does not prove the absence of disease. It only proves that you are looking with inadequate tools.
One of the article’s most serious mistakes is this: it confuses the absence of a simple clinical test with the absence of organic disease.
And that mistake has caused harm for decades.
The article also says:
“Almost $2 billion and half a decade of international effort have yielded little more than hypotheses about micro blood clots and spike proteins and mitochondrial dysfunction.”
No. That is not correct.
A hypothesis is a provisional explanation. But when you compare patients and controls and find significant differences in muscle tissue, metabolism, response to exertion, immune biomarkers, viral antigens, autoantibodies, or vascular dysfunction, you are no longer talking about “little more than hypotheses.” You are talking about lines of biomedical evidence that still need to be organized, replicated, stratified, and translated into treatments.
That is not scientific failure. That is research into a complex and new disease.
🔵Continued in the next post.👇🏻
(1/6)
Check out these talk summaries from our recent PolyBio Symposium👇
Highlights include that four groups — Tim Henrich (UCSF), Marcus Buggert (Karolinska), Nicolas Huot (Institut Pasteur), and Esen Sefik (Yale) — presented different lines of evidence (human gut biopsies, non-human primate models, humanized mice) all pointing to the same conclusion: SARS-CoV-2 persists in #LongCovid gut tissue and adjacent lymphoid structures, and that persistence drives ongoing immune dysregulation.
Many with #MECFS and #LongCOVID experience #dysautonomia- which can greatly affect daily life. With proper management, symptoms like dizziness and rapid heart rate can be improved. See our new orthostatic intolerance overview by Dr. Hoppers! ➡️https://t.co/iMX0kA7BNc
@OpenMedF
Excited to be visiting @VirusesImmunity at the 2nd @YaleCII symposium today to talk about #LongCovid - Where we are, where we need to go, and how we can get there.
Long COVID is destroying millions of people's career paths and lives. Imagine the devastation of working your way up to your dream job for decades and having to let it go because of #LongCovid@JenCalfas and @poverberg report in the @WSJ
https://t.co/OIQbZCVCoS
For too long, millions of Americans suffering from long COVID have had their symptoms dismissed or ignored – by the medical community, by the media, and by Congress. Unacceptable.
Congress must act now. Yes. It is time for a Long Covid Moonshot.
@hubermanlab can we please do an episode on #LongCovid? According to the CDC, at least 7% of the US population (with similar numbers globally) now report struggling with Long COVID. There’s a lot of knowledge we could share to help.
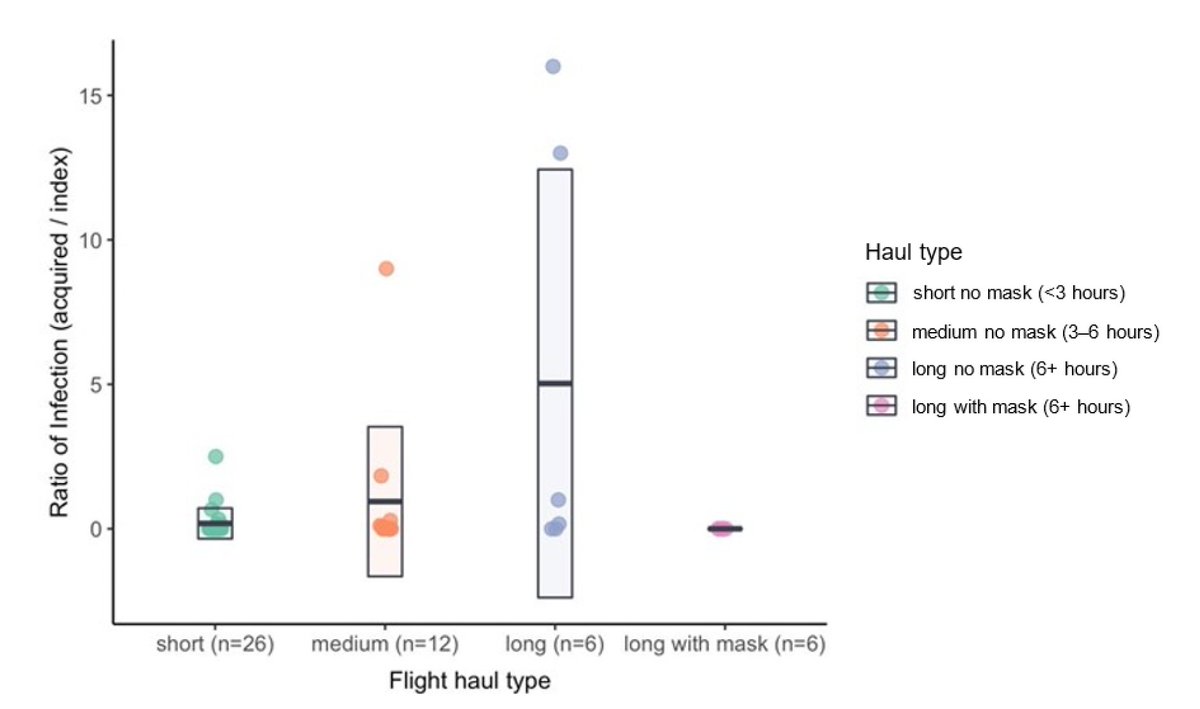
A systematic review of airplane flights and Covid infections: duration of flight correlated with infection risk, long flights> 6 hours markedly increased risk (25X) and mask use blocked them
https://t.co/KIdLgKB1zV
h/t @linseymarr
We are proud to have supported this new paper published in @BrainBehavImm.
Led by @MBVanElzakker & team at @MGHMartinos, it is the is first study to document neuroinflammation in the long COVID brain along with evidence of vascular problems: https://t.co/KsVN4eJ4Kf
Downright incredible — no way this happens without these collective efforts.
Thank you everybody who chose to use your limited energy to do something to help the #LongCovid community 🙏
Tell @ChrisCuomo that 33 scientists from 14 institutions joined forces to write this paper documenting evidence for #SARS-CoV-2 persistence as a potential driver of #LongCOVID. We call for more clinical trials of drugs capable of clearing persistent virus: https://t.co/IKccdqJKkn
This is an excellent session on where we are now with LC, from top researchers with deep clinical perspective. There's a long way to go, but I'm hopeful.
This was a terrific session on #LongCovid, by 3 international leaders in LC. We've made significant progress in understanding the causes of the disease & the epidemiology, but still lack evidence-based therapies. Hope that changes soon. Available here: https://t.co/LV3EWxYjQ0