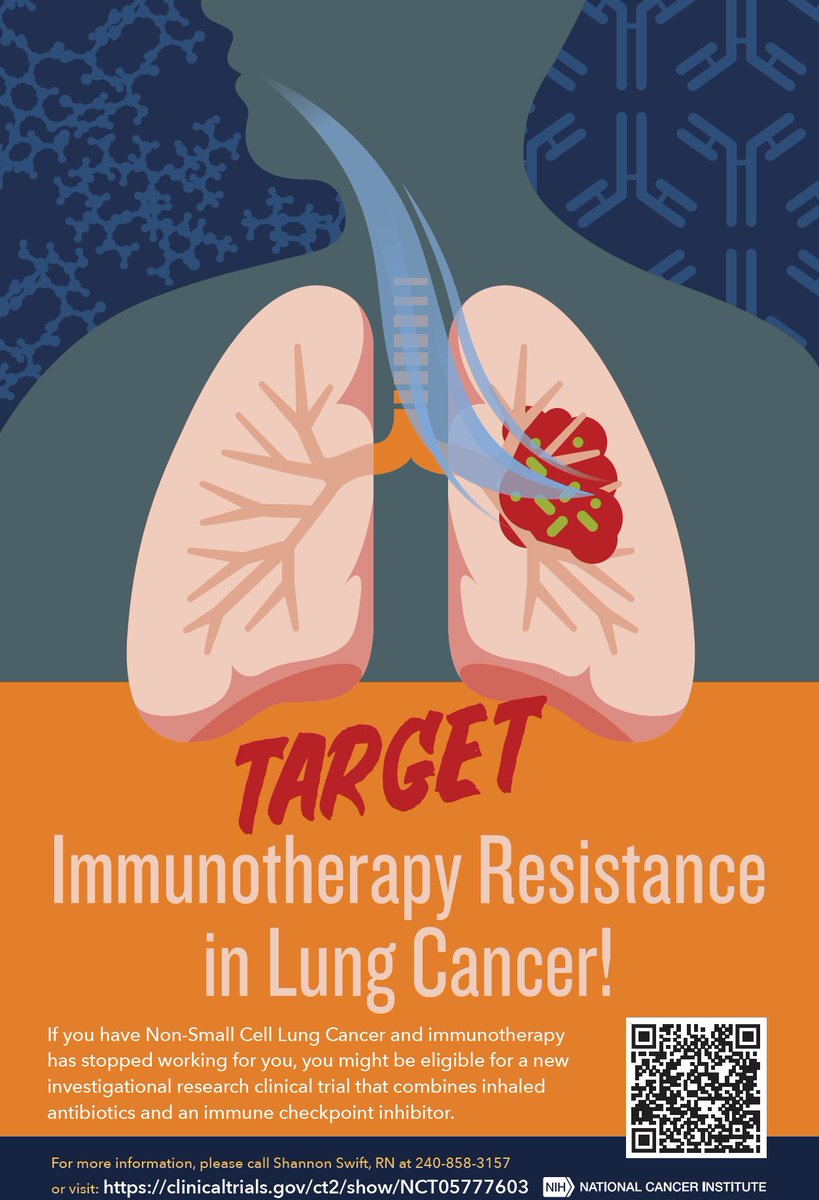
We are very excited to bring our strong pre-clinical findings to patients! This trial is for #immunotherapy resistant #NSCLC. No insurance is needed and ✈️🛏️ will be provided! Check out 👉https://t.co/fwq77L97qi
🫁 Peroperative immunotherapy treatment for NSCLC 🫁
🌟 A summary of current clinical data.
�� This will make it easier to create future updates.
#LCSM
#nsclc
#perioperative
Phase 3 CheckMate 73L @NatureCancer showed introduction of nivolumab with concurrent chemoradiation followed by nivo+ipi consolidation for stage III NSCLC did not improve OS over standard consolidation durvalumab & had higher rates of pneumonitis.
https://t.co/GRrqQQpnf1
🫁 MAPI in stage I LUAD.
A multiomics metabolic-associated prognostic index (MAPI) outperformed clinicopathologic features and prior signatures for risk stratification in stage I LUAD.
High-risk tumors showed stemness, immune exclusion, metabolic rewiring, and lower predicted immunotherapy sensitivity.
Potential therapeutic signals: paclitaxel, bortezomib, vincristine.
📖 @JCOPO_ASCO
DOI 👉🏻 https://t.co/yhPmLUVgAJ
#CánCare #LUAD #NSCLC #lcsm #biomarkers
Online here: https://t.co/nzzWChWPkD
Open access here: https://t.co/MEUA5HUeGx
Key supporters of this work are @CR_UK , @CRUKLungCentre , @UCLHresearch alongside many others
Impact of 1L amivantamab + lazertinib vs osimertinib on acquired resistance in EGFR mutant NSCLC @JTOonline. Ami/laz reduces MET amp (3.4% vs 13.1%) and acquired EGFR resistance mts (1.4% vs 7.6%). 2L PFS longer in ami/laz arm vs osi (8.4m vs 5.3m).
https://t.co/UYIfOrJEmZ
Proud to be part of #NCI and to lead one of these immunotherapy trials. Nothing is more rewarding than seeing a patient respond well to a treatment you helped develop!
So proud of the many decades of the NCI’s funding discovery science and translational research that is led to such marked improvements for patients with cancer.
#YourNCI
https://t.co/hTS4QTqbsp
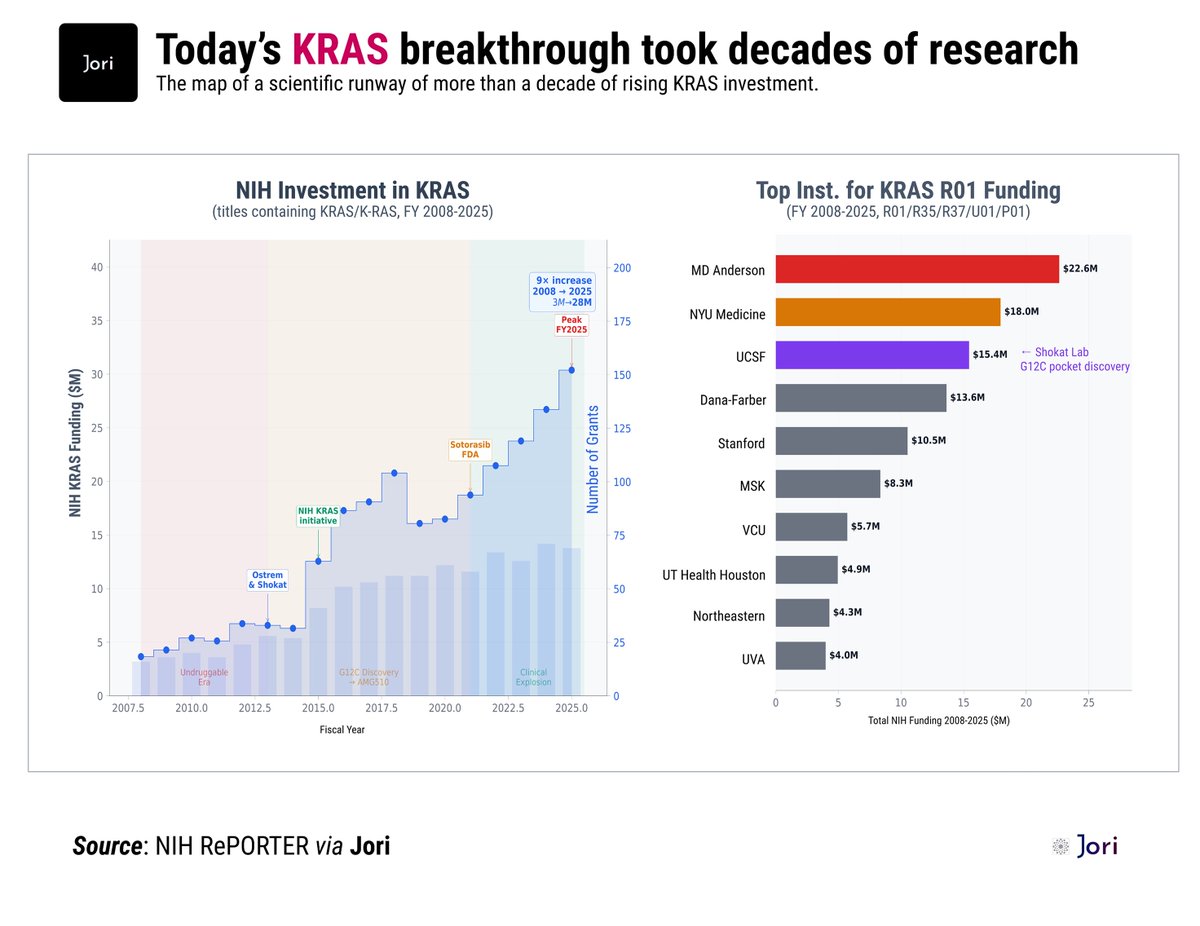
Today’s KRAS win didn’t start today.
It took decades.
Daraxonrasib nearly doubled survival in pancreatic cancer. That’s extraordinary!
But lets zoom out for a sec:
▪️KRAS was called “undruggable.”
▫️NIH quietly poured ~$172M behind it.
▫️Funding grew 9x.
💡One insight (Shokat lab, 2013) changed everything.
This is how breakthroughs are supposed to work:
public money → basic insight
academic labs → first leap
industry → drug + survival curve
Today’s headline has MANY authors.
Congrats to @Revolution_Med and every scientist who stayed on KRAS when it looked impossible.
🎈this is what compounding science truly looks like
= = = = =
Source: NIH RePORTER via @Jori_health
= = = = =
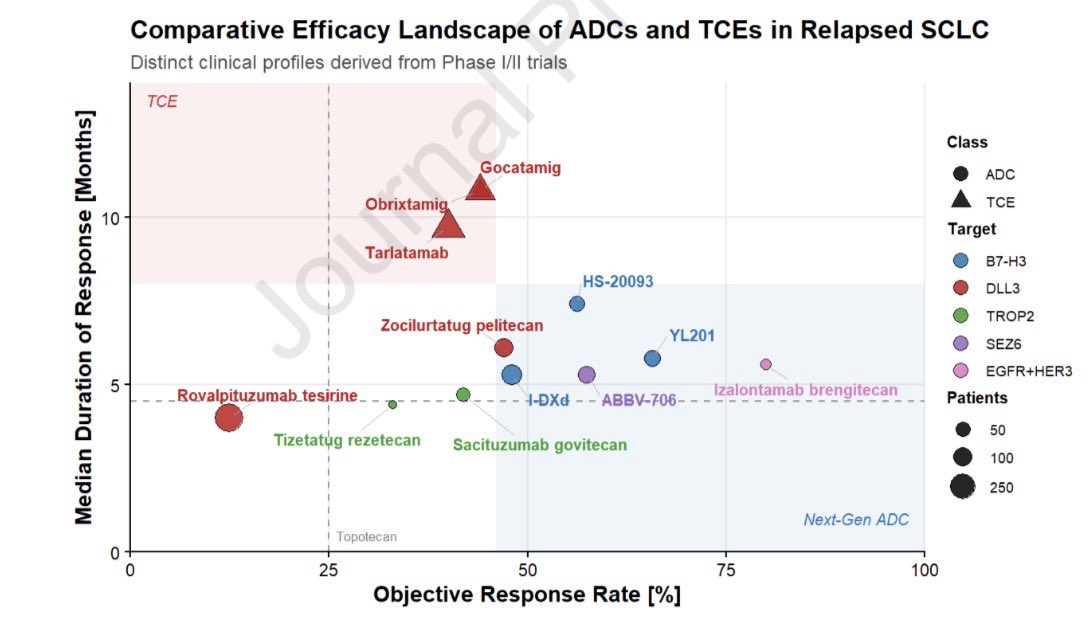
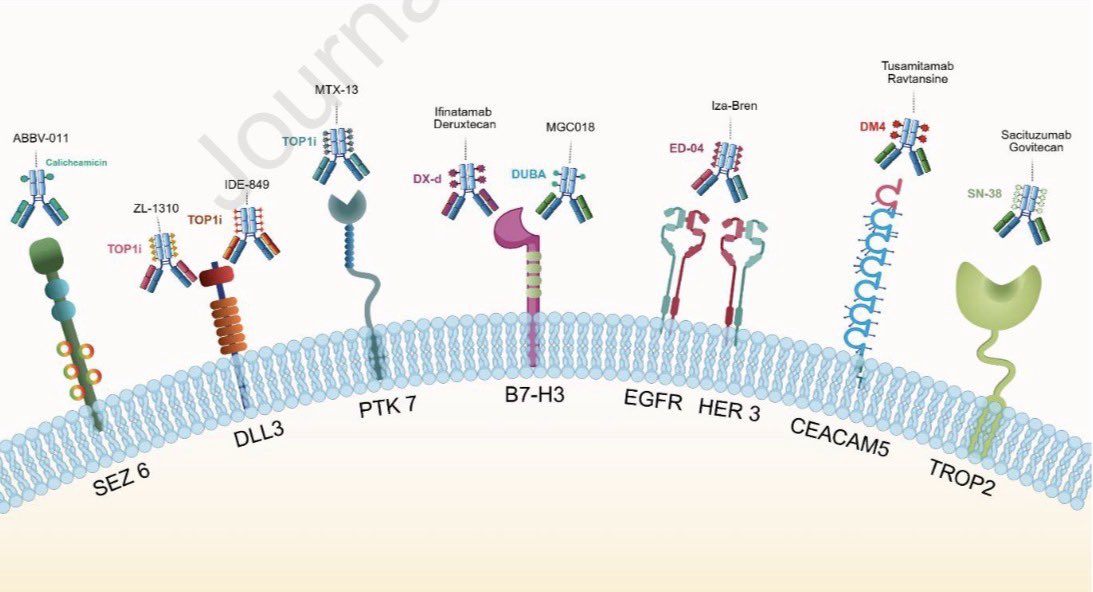
📄 Our review in @JTOonline is now out: Antibody–Drug Conjugates in Small-Cell Lung Cancer: DLL3, B7-H3, TROP2 and Beyond
DOI: 10.1016/j.jtho.2026.103726
Key question: not just whether ADCs work in relapsed #SCLC, but how to sequence them with DLL3-directed T-cell engagers.
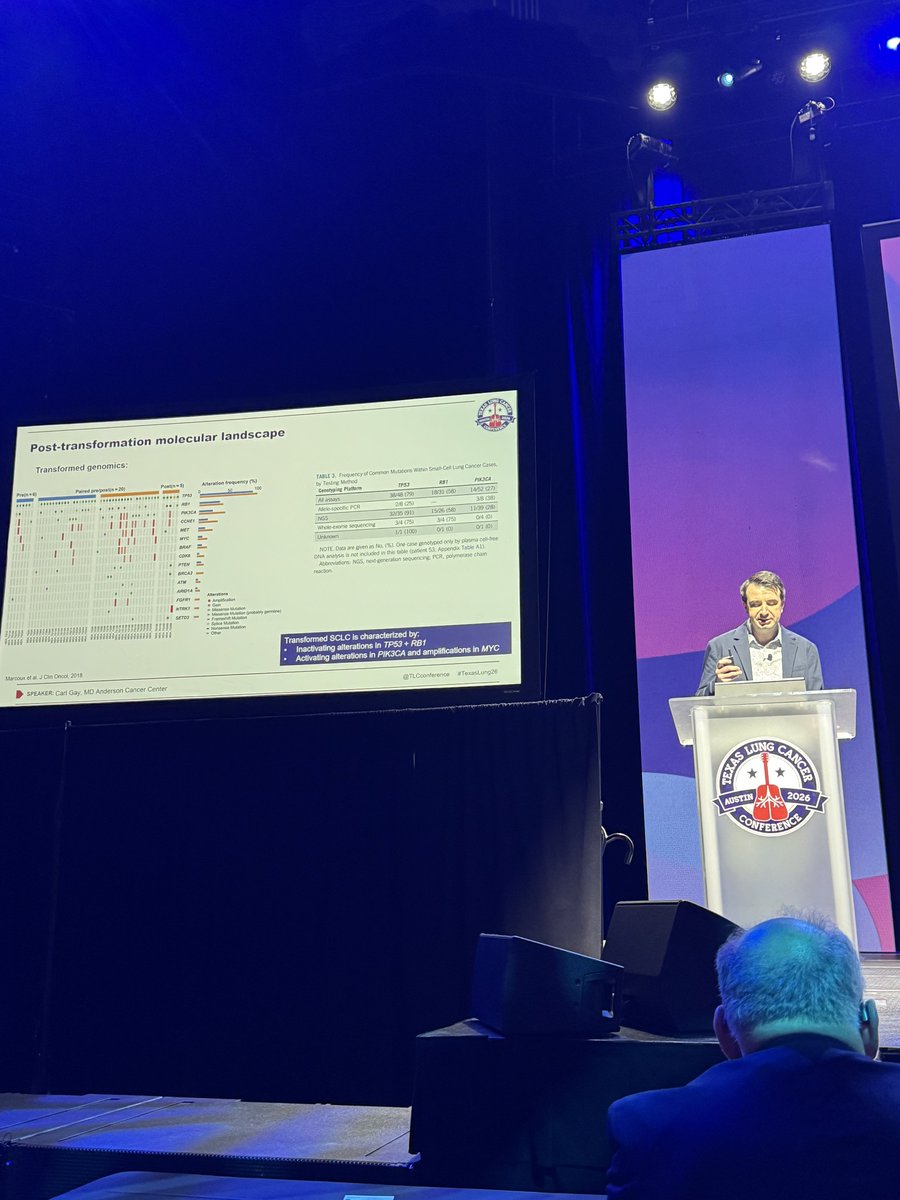
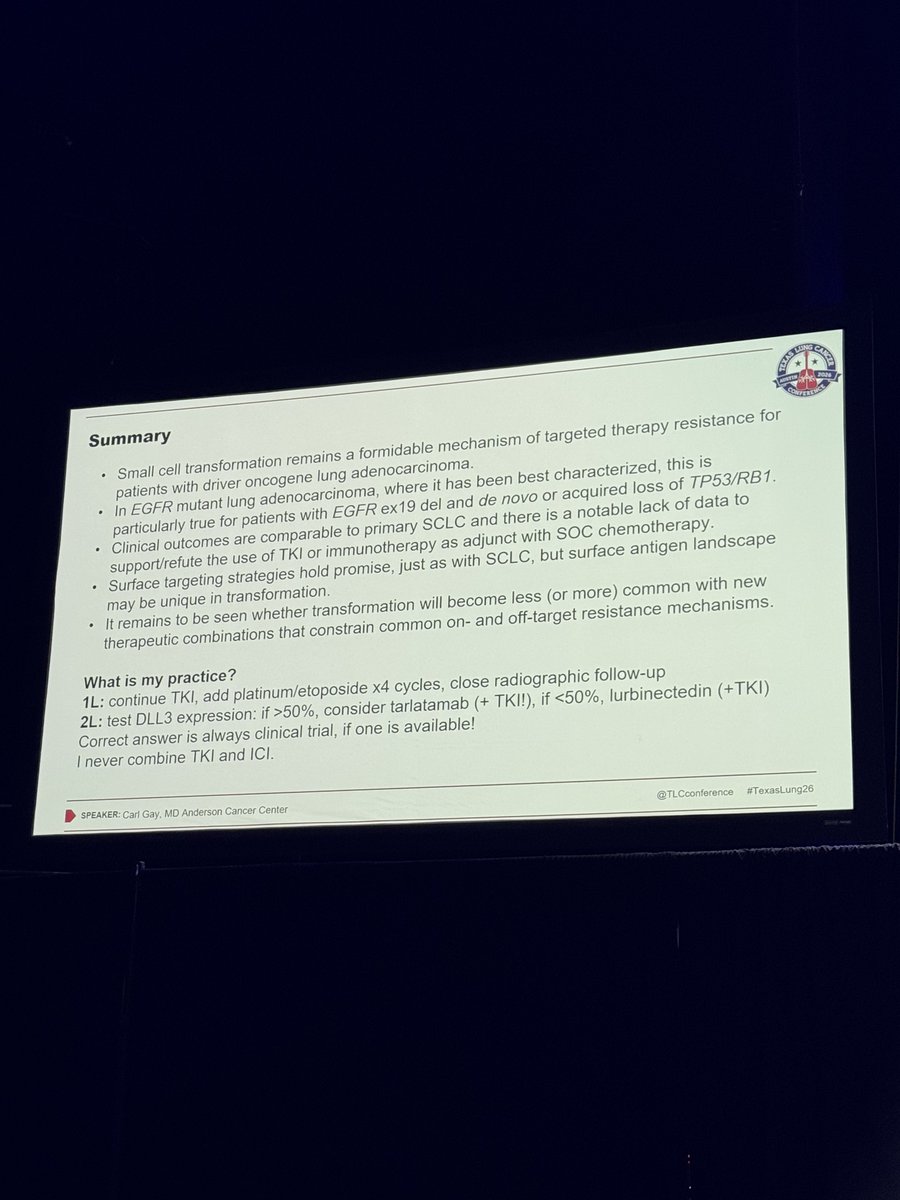
EGFR+ NSCLC to SCLC: what to do today?
1. Prioritize clinical trial
2. If no trial, chemo + TKI
3. Tarlatamab not the "blockbuster" solution for most pts but DLL3 expression might help us
#TexasLung26
Real-world data on RET inhibitor retreatment; retrospective and small sample size. Support switching after toxicity, while highlighting only modest and selective benefit after progression.
Value of retreatment with alternate selective RET inhibitors in NSCLC discussed @CCR_AACR. When one agent discontinued for toxicity, switching to an alternate had RR 67%, mPFS 9.9m but AEs re-occurred in 64%. When switched due to toxicity, RR 23%, PFS 7m.
https://t.co/XpLu6uGU9B
This further confirms the differences of single amino acid mutation in the same molecule. Same as difference between Kras G12C and G12D. One more point: oncogenic mutations do not mean poor responses to ICI. The story with EGFR mutations and ICI are very different...
Should we do molec testing on all NSCLCs? Answer: YES @JTOonline
- 82328pts
- 35.1% AGA+ (adeno=45.8% adenosq=40.9% sarcomatoid=29.1% NOS=27.6%, LCC=21.1% sq=6.5%)
- age, sex, region assoc seen
Congrats @Al3ssandroRusso@ChristianRolfo@oncoalert#LCSM
https://t.co/M3bDWxZA7U
This is an important read - and a key response to this challenge is to concentrate resources on early trials for the deep molecular profiling of responses to novel therapies- and advance programs only if biology aligns with pathological/clinical responses
I asked ChatGPT : "what happens to nations invest more in the military than in science", it replied: “the fall of great empires — from Rome to the Ottoman Empire — always involved prioritization of force over knowledge, conquest over curiosity.” https://t.co/AXVJzpUby4
Phase III EXCLAIM-2 trial of 1L mobocertinib vs chemotherapy in #EGFR exon 20 NSCLC @JCO_ASCO. Negative trial: PFS 9.6m in both arms (HR 1.04). RR 32% with mobocertinib and 30% with chemo. Mobocertinib also had 20% G3+ diarrhea. PAPILLON remains standard.
https://t.co/UmNpXAUimv
CHRYSALIS-2 Cohort A: amivantamab + lazertinib in #EGFR NSCLC after osimertinib and chemotherapy @JTOonline (n=162). BICR RR 35%, CBR 58%, DOR 8.3m, PFS 4.5m, OS 14.8m, and CNS efficacy noted. AEs included rash in 81% (G3 10%), paronychia in 52%.
https://t.co/rbobOcx1In
Great slide presented tonight by @LudaBazhenovaMD reminding us that it's no longer sufficient to know what street the EGFR mutation lives on, but instead what address it lives on so we know which TKI to prescribe.
😱Autoreactive CD8 + T cells are NOT DEPLEATED in the thymus during negative selection, instead, they are evicted from the thymus, where mechanism of peripheral tolerance controls their activation.
https://t.co/sEs3otWoY6
@ScienceMagazine@NIH