Assistant Attending, MSKCC, Genitourinary Oncology Service
Tweets are my own opinions and do not represent the views or opinions of Memorial Sloan Kettering
🧬 What happens to Nectin-4 expression after EV+pembro? New paired biopsy data from @MichalSternsch@MSKCancerCenter at #ASCO2026: some tumors retain membranous Nectin-4 post-EVP — complete target loss is seen in some cases of early progression - and in 6/6 post EV/P tumors at cystectomy Nectin-4 expression decreased in residual tumors. | Abstract 552910, Poster A56 #BladderCancer
Selecting the right ADC for the right patient will increasingly depend on biomarkers, especially with so many ADCs sharing similar payloads.
Led by @BarbaraPistill2, we discussed this challenge and the need for better biomarkers in our @cancercell review
https://t.co/Ajv7tjT2EF
Impressive data.
> 500 ADCs in preclinical development in China
The field is now moving towards dual-target and dual-payload strategies. Very promising!
Impressive results from a phase 3 trial of Iza-Bren (anti-HER3/EGFR TOPO1 ADC) vs chemo in pretreated mTNBC, with improvement in PFS and OS. High rate of hematologic toxicities, including 5% febrile neutropenia. Phase 3 ongoing to confirm these results in a global population.
CaboNivo final results in non-clear cell RCC presented by Dr Darren Feldman: ORR 43% in Cohort 1 (papillary, unclassified, tRCC), with a striking 88% ORR in FH-deficient RCC. mPFS 11 mo, mOS 28 mo. No responses in chromophobe RCC. CaboNivo confirmed as a standard 1L option for these rare subtypes. #ASCO26 #RCC @OncoAlert@ASCO@OncBrothers
Really interesting work from @MichalSternsch@Dr_Aggen showing paired tissue analysis of Nectin4 pre- and post-EVP.
39% primary and 49% acquired resistance, with a trend towards ⬆️Nectin4 loss in primary cases suggesting possible different mechanisms of resistance.
@OncoAlert
@MichalSternsch also carefully profiled mNectin-4, cNectin-4, TROP2, and HER2 in post EV/P tumor samples. These data support that some patients need different targeted ADCs (TROP2 and HER2) and others need NECTIN-4 targeting with a different payload.
🧬 What happens to Nectin-4 expression after EV+pembro? New paired biopsy data from @MichalSternsch@MSKCancerCenter at #ASCO2026: some tumors retain membranous Nectin-4 post-EVP — complete target loss is seen in some cases of early progression - and in 6/6 post EV/P tumors at cystectomy Nectin-4 expression decreased in residual tumors. | Abstract 552910, Poster A56 #BladderCancer
@MichalSternsch talking with @Uromigos about our work on mNectin-4 expression post EV/P. Early signal suggests mNectin-4 expression changes drive resistance in some patients early, but in other cases of late or acquired resistance nectin-4 is retained. #ASCO26
🔬 Exciting work from @MSKCancerCenter at #ASCO2026! Aditi Gupta shows that EV+pembrolizumab drives early peripheral T cell activation in metastatic urothelial cancer — and CD8+ CTLA-4 expression may predict response. 🧬 | Abstract 542284, Poster A50 #mUC#Immunotherapy #BladderCancer
🔄 Can you rechallenge with Enfortumab Vedotin after progression? New real-world data from @MichalSternsch@MSKCancerCenter at #ASCO2026 says: in some yes - promising in patients with prior EV benefit & EV-free interval >6 months. 📊 55 pts, ORR 25%, median OS 15.2 months. | Abstract 547088, Poster A57 #mUC #BladderCancer #Immunotherapy
#ASCO26 GU Oncology Spotlight 🚨
🔬 Management in Bladder Cancer After Pathologic Complete Disease Response
Presented by Brendan J. Guercio, MD
@OncoAlert@ASCO
In muscle-invasive bladder cancer, pCR after neoadjuvant therapy is one of the most powerful prognostic signals we have.
But the key clinical question is becoming more complex:
➡️ If a patient achieves pCR after perioperative therapy, should we continue adjuvant treatment — or stop?
Historically, pCR after neoadjuvant chemotherapy has been associated with excellent outcomes.
In SWOG 8710:
• pT0 after neoadjuvant chemotherapy → ~85% 5-year OS
Meta-analyses also support pCR as a strong positive prognostic marker for recurrence-free survival.
So pCR matters.
But pCR is not the same as proof that postoperative therapy is unnecessary.
📌 Current MIBC perioperative landscape is changing fast
For cisplatin-ineligible or cisplatin-declining patients:
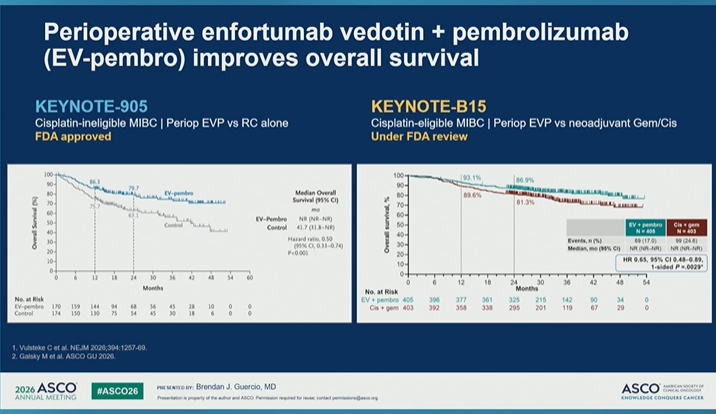
• KEYNOTE-905 / EV-303: perioperative EV + pembrolizumab is now a major standard-setting approach
• VOLGA: perioperative EV + durvalumab ± tremelimumab adds another immune/ADC-based strategy
For cisplatin-eligible patients:
• NIAGARA: Gem/Cis + perioperative durvalumab improved outcomes
• VESPER: ddMVAC improved survival vs Gem/Cis but with greater toxicity
• KEYNOTE-B15: perioperative EV + pembrolizumab improved OS vs Gem/Cis-based treatment
The field is clearly moving toward immunotherapy-based “sandwich” regimens.
🧭 Management after pCR: continue or stop?
Current standard practice remains:
➡️ Continue planned adjuvant therapy for perioperative sandwich regimens, regardless of pathologic response.
Examples:
• NIAGARA: resume durvalumab post-cystectomy
• Perioperative EV + pembrolizumab: resume planned postoperative therapy
• Cisplatin-based chemo alone with pCR: surveillance remains standard
Why?
Because we still do not know the relative contribution of:
🔹 the neoadjuvant component
🔹 the postoperative/adjuvant component
🔹 surgery
🔹 pathologic response itself
🔹 underlying tumor biology
⚠️ Unanswered question
Can adjuvant therapy be safely de-escalated based on pCR?
Not yet.
pCR is prognostic.
But we still need prospective evidence to determine whether it is predictive enough to guide treatment discontinuation.
This is especially important because postoperative therapy may add:
• toxicity
• neuropathy
• immune-related adverse events
• treatment burden
• cost
• delays in recovery
• impact on quality of life
💬 My take
pCR is an excellent sign — but it is not yet a permission slip to stop planned adjuvant therapy after modern perioperative regimens.
For now, the safest message is:
➡️ follow the regimen as tested
➡️ discuss toxicity and recovery
➡️ avoid unproven de-escalation outside trials
➡️ develop biomarkers that can identify who truly needs postoperative treatment
The next frontier in MIBC is not only achieving pCR.
It is learning how to use pCR — together with biomarkers and patient outcomes — to personalize escalation and de-escalation.
@DrChoueiri 🇺🇸@hoperugo 🇺🇸 @matteolambe 🇮🇹 @TiansterZhang 🇺🇸 @CathyEngMD 🇺🇸 @stolaney1 🇺🇸 @montypal 🇺🇸 @tompowles1 🇬🇧 @brian_rini 🇺🇸 @cdanicas 🇪🇸 @NiuSanford 🇺🇸 @amerseburger 🇩🇪 @GlopesMd 🇺🇸 @Icro_Meattini 🇮🇹 @PGrivasMDPhD 🇺🇸 @DrYukselUrun 🇹🇷
@ecancer@urologysummit@UrologyTimes
#ASCO26 #GUOnc #BladderCancer #UrothelialCancer #MIBC #pCR #EVPembro #Immunotherapy #PrecisionOncology
Data on nectin-4/Topo-1 ADC (LY405) #ASCO26. @IyerGopa RR= 42% (n=48). RRs are maintained after prior Nectin-4 targeting but not after prior Topo1 payload exposure. Resistance is therefore mainly payload orientated. Sequencing Nectin4 ADCs requires R3 trials, but look imporant. LY405 is metabolized by CYP2D6. Absence of CYP2D6 (~10%) led to serious toxicity. Measuring CYP2D6 is straightforward but important for this drug . @OncoAlert
LY405231 a topo-I nectin-4 targeted ADC retains clinical activity post EV/P. Presented by @IyerGopa#ASCO26
➡️ ORR 42%
➡️ Prior Topo-i exposure 0% (0/18 responses)
➡️ Increwased toxicity in the 7% of patients with low CYP2D6 activity score - one of the first markers of increased toc with a topo-I drug
One of the most important take away from EV302 follow-up - 83.6% of pts with a complete radiographic response are alive at 42 months in follow-up
For these patients we should advocate for surveillance cystoscopies for patients with in tact bladders +/- CNS imaging annually. #ASCO26
REGISTER for our NRG-GU015 "ARCHER" site webinar discussing the study assessments for the trial studying shorter duration RT for patients receiving chemotherapy for bladder cancer. This webinar will be June 9th at 1:00PM ET. Register at https://t.co/oiS6Z4RrP2