1/21
Acid–base interpretation often feels like a maze.
But there’s a simple way to make sense of it at the bedside.
It starts with pH, strong ions, and base excess.
1/
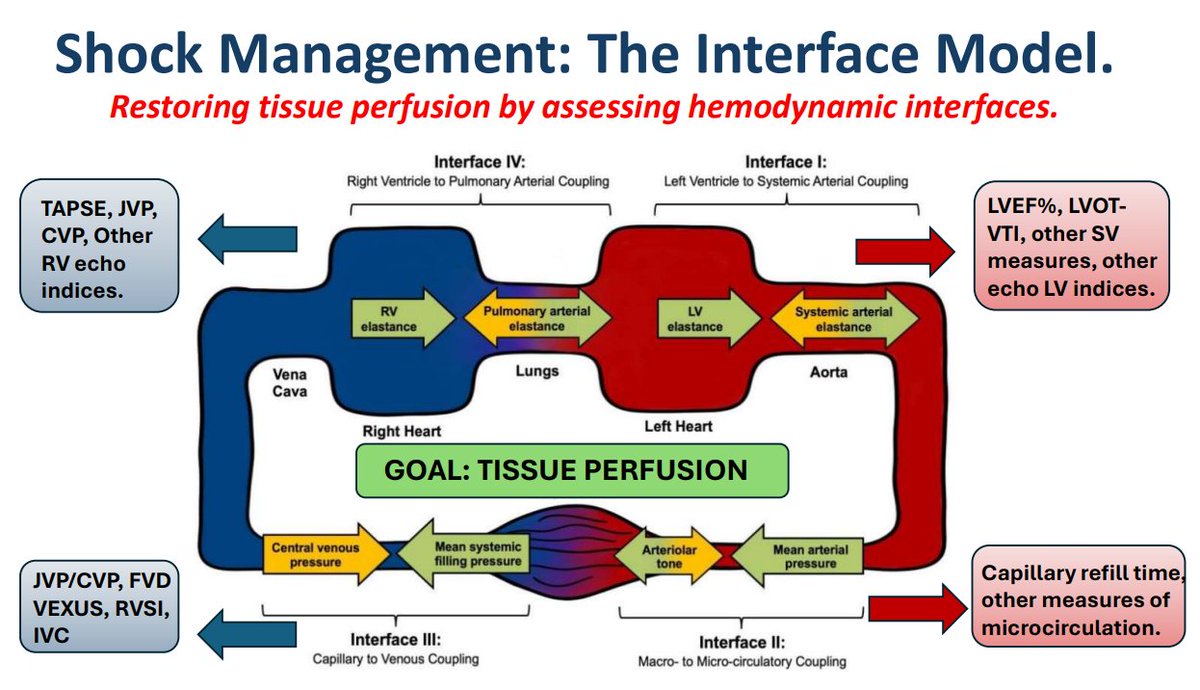
Shock is complex. But our tools are often simplistic.
This paper proposes a new model:
🩸 Four circulatory interfaces that must stay coupled to maintain perfusion.
Uncouple any one — and shock worsens.
#Shock#MedX#FOAMcc
Here’s the framework.
🔗 https://t.co/8xxEcdzYUw
🧵 Starling’s Law: Misunderstood, Misapplied, and Still Misleading
1
🚨 “Starling’s Law explains how the heart increases cardiac output.”
You’ve probably heard this a thousand times.
But it’s wrong.
Or at least - very incomplete.
Let’s fix it.
Because this matters - for heart failure, fluids, vasopressors, inotropes, afterload, and how we think about the whole system.
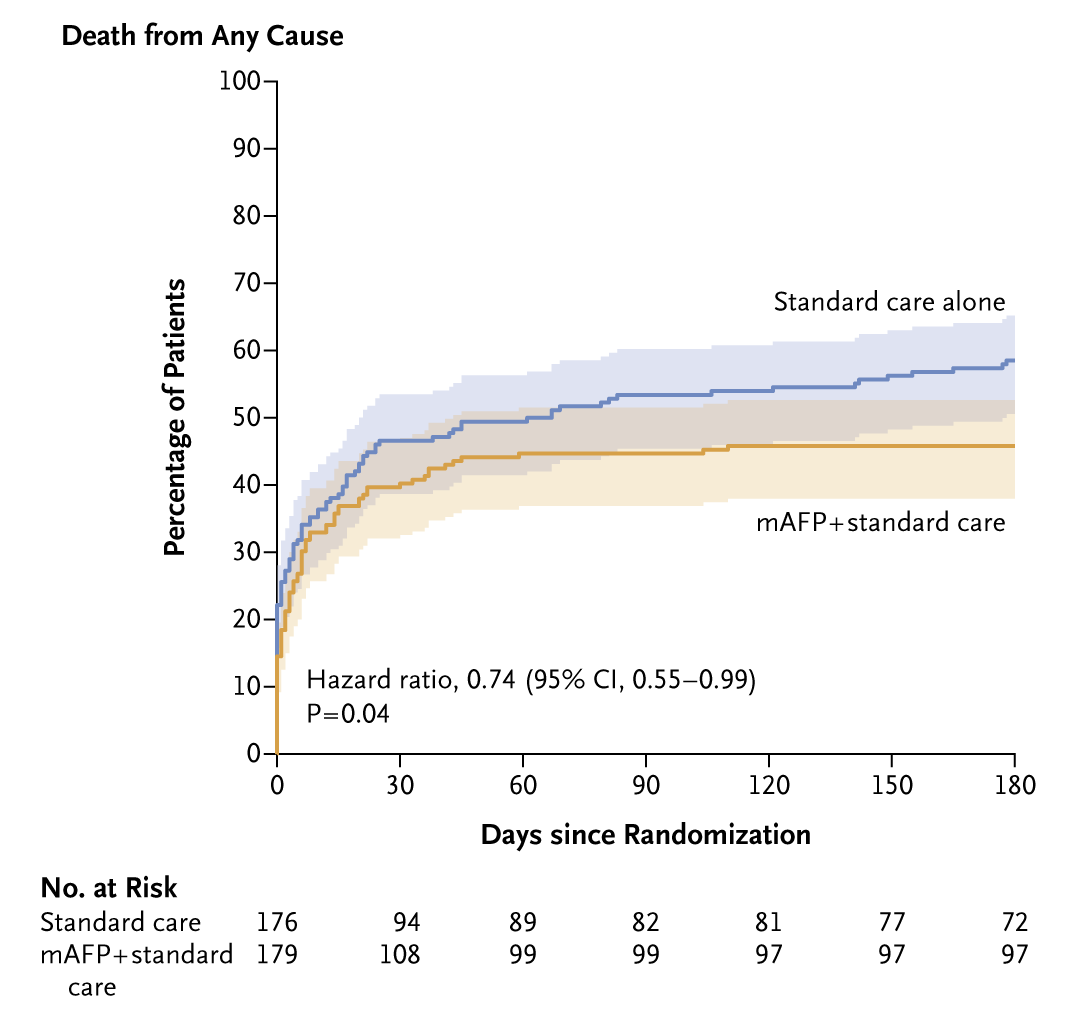
Presented today at #ACC24:
In the DanGer Shock trial involving patients with STEMI and cardiogenic shock, mortality at 6 months was lower with mechanical circulatory support with a microaxial flow pump than with standard care alone. Full trial results: https://t.co/3625asvzu8
A day in the life of @drttinglow who makes multitasking look so easy 💪🏻
Thanks for flying the #NUHCS flag high-we are lucky to have you as a great doctor, amazing colleague & honest friend!
#wic#womeninmedicine#internationalwomensday#iwd2022 https://t.co/3NKZwGQlor
Pleased to share our letter @TheLancetRheum arguing that severe COVID-19 is a virus-independent immunothrombotic process. https://t.co/8qJzFPrgkq describe
@Jopo_dr Would argue that it was never silent hypoxia but rather silent hypoxemia. Patient unaware of low O2 sats. No evidence that patients were indeed hypoxic. Commonly seen in pulmonary vaso-occlusive physiology when both SaO2 and SvO2 low, but ⬆️tissue extraction maintains tissue O2.
@farid__jalali @WesElyMD@gattinon@Acute_Pulmo_Med@robertpdickson @ColinRCooke https://t.co/nsj2PnpZ7g this paper showed lack of topological correlation between lung pathology and viral presence in alveoli. Consistent data.
coding department: Could you clarify whether this patient had a STEMI or an NSTEMI? The chart says both.
me: actually the STEMI/NSTEMI pardigm is profoundly flawed, I’d classify this as an occlusive MI
coding: there’s no code for that
me: precisely
coding:
me:
@FrankS1956 @connors_md @PittHealthSci@PACCM@JerryKrishnan Thanks; is it possible that the group was self-selected to have low risk of events due to the time delay involved in randomisation and Rx initiation (median 7+3 days from Dx)? 0.5% event rate appears too low for a mostly non-vaccinated group with median age 54.