@gregmushen@GuruAnaerobic Agree. Im not super ‘moved’ by this study. W/ a wrist worn accelerometer, chopping vegetables could register as MVPA and cycling might be missed. Tracking period was 7 days, assumes stable activity (and CRF) for 7 years. Accelerometer + questionnaire >>> either alone.
@BowTiedPhys This conclusion relies on a 7 day tracking period and assumes stable CRF, which was estimated via a protocol with R^2 of ~0.5 and RMSE of ~4.8 mL/kg/min. Periodic use of a brief questionnaire, even just during the tracked 7 days, would have added a lot of value imo.
I read your substack on this topic. Where I agree with you: [a] defining VO2max vs VO2peak is subject to variability at the investigator level, [b] social media is probably causing excessive attention on VO2max and not enough on performance or CRF more generally, [3] evaluating performance on an established treadmill protocol offers a lot of value and with a much lower barrier of entry relative to VO2max measurement (indirect calorimetry). I don't think we'll ever align on the degree to which VO2max offers value, but reasonable minds can disagree. Thanks for taking the time to write the substack and for making it available.
@ChrisMasterjohn@PeterDiamandis Counterpoint, respectfully: Peak METs are a validated measure of cardiorespiratory fitness, especially when derived from maximal or symptom-limited exercise testing.
Do you think direct VO2 measurement would materially change the association?
@nicknorwitz Agree there is nuance and heterogeneity in effects at the individual level. However, respectfully, i think your synthesis under emphasized the associative data we have regarding potential protective effects.
@bryan_johnson Data on mortality during COVID in relationship to CRF level, categorized by condition. Putting aside chronic sleep deprivation, you get more benefit per dose with exercise than probably anything else and it's not even close imo.
POV, you're a doctor trying to advocate on behalf of your patient for insurance coverage
Start 10:30 AM
-Wegovy denied by Aetna after being covered and after patient achieved clinically meaningful weight loss.
-Authored LOMN which included patient's starting weight, obesity related comorbidities, total weight loss percentage, and rationale for medical necessity (risk of weight regain and health complications if medication not covered, general health benefits associated with maintaining optimal weights).
-Appeal on basis of LOMN was denied, only explanation provided --> not medically necessary.
-Pt called insurance, was told that the information provided in the LOMN authored and signed by the doctor (me) is generally what they need, but a peer-to-peer (phone conversation with a "doctor" representing the insurance company) is required in order to potentially provide coverage.
-I call insurance, provide the patient's information and select number option for appeal, hold for 10 minutes, reach someone, then confirm patient info with them and reason for the call, and the representative tells me I need to call a different number to reach the correct department.
-The above happened again with the second department, and then again with a third department
-Speaking with 4th department, first person then transferred me to a pharmacist.
-The pharmacist (CVS Caremark Rep) said there was no record of the LOMN I authored, I offered to share the reference # provided to me by our pharmacy liaison team, pharmacist said he cannot use the reference # to look it up.
-I offered to email (with encryption given HPI) the LOMN, he said it must be faxed.
-I faxed it while still on the phone, and requested to stay on the phone while he views the faxed LOMN, he said that is not possible, that he can call me back.
-Called patient back and provided these updates.
End 11:15 PM.
@mcuban
@iruletheworldmo This article summarizes what has been learned since @ezraklein wrote on 3/12/2023 "The coders casting these spells have no idea what will stumble through the portal", https://t.co/IDM0tHZvLV. Equal parts fascinating and frightening
@DeanTTraining What are your thoughts on using this a pec fly machine with one arm at a time and crossing midline at the end of movement. Better sternal head activation that way or not much of a difference relative to two arms at once.
@DeanTTraining I explain it to patients with a metaphor. In golf on a single hole, 3 bad shots in a row can be nullified with an excellent 4th shot (chip in from sand). Weight is regulated unfortunately in the opposite.
Medicare recipients (~20% of US population) did not have coverage for telemedicine appts during the shutdown. In-person appts were covered but transportation can be difficult for those > 65 yo and medical offices can accommodate a limited number of providers on a given day. That was a major healthcare access issue for a vulnerable group of people.
@Wegiveyouhealt1 Counterpoint: Everything in the universe "runs" according to mathematical formulas. Any suggested exceptions are processes that we don't understand well enough yet.
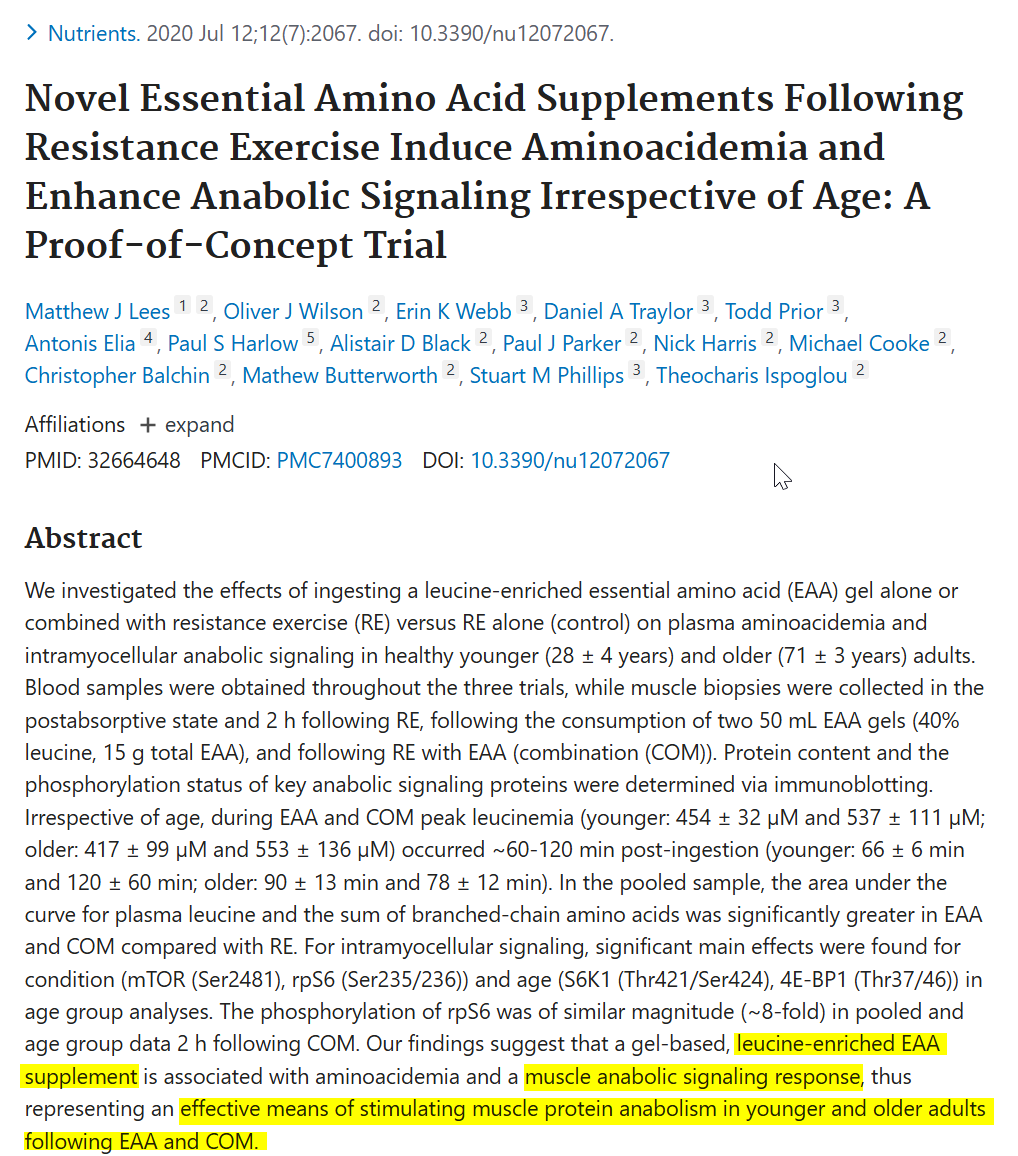
@brady_h Putting gary aside, there's at least a few studies that demonstrate MPS benefit in association with essential amino acid supplements. Review article on the topic: https://t.co/rapOlgyCIa
Use your favorite LLM/AI and ask it to summarize the evidence on nattokinase. I think you'll find that the overwhelming majority of evidence reveals no benefit for reducing risk of defined clinical outcomes (heart attacks and strokes) and its use can cause bleeding. Worth noting that original poster promotes a 20% discount for nattokinase on their linktree page, which leads me to conclude that he has a financial relationship with a company that sells nattokinase.