Medical Oncologist focused on GI & Endocrine Malignances. Vall Hebron University Hospital. Vall Hebron Institute of Oncology (VHIO). Teknon Cancer Institute.
Honored to have participated in the Revolution RAS-302 clinical trial that demonstrated 60% overall survival for patients who received the KRAS on inhibitor #Daraxonrasib compared to chemotherapy.
Our team @panoncology participated in this practice changing clinical trial in 🇵🇷 Puerto Rico. We are grateful to @RevMedicines and their leaders, scientists Dr Jan Smith, Dr. Wang, Dr. Salman, and oncologists Miguel Colon Donate, Karina Arocho, Luis Velazquez, Rafael Perez Casellas, Santa Merle, Radiologist Dr. Rafael Vicens and All PanOncology team members. Thank you to our partners Doctor’s Center Hospital Orlando Health and IGM Oncologic Hospital in 🇵🇷
We are privileged to have the trust of our patients, their, families and our colleagues who work together and support clinical trials to advance the science and cure cancer #RAS302 #ClinicalTrials #ASCO26 #PancreasCancer
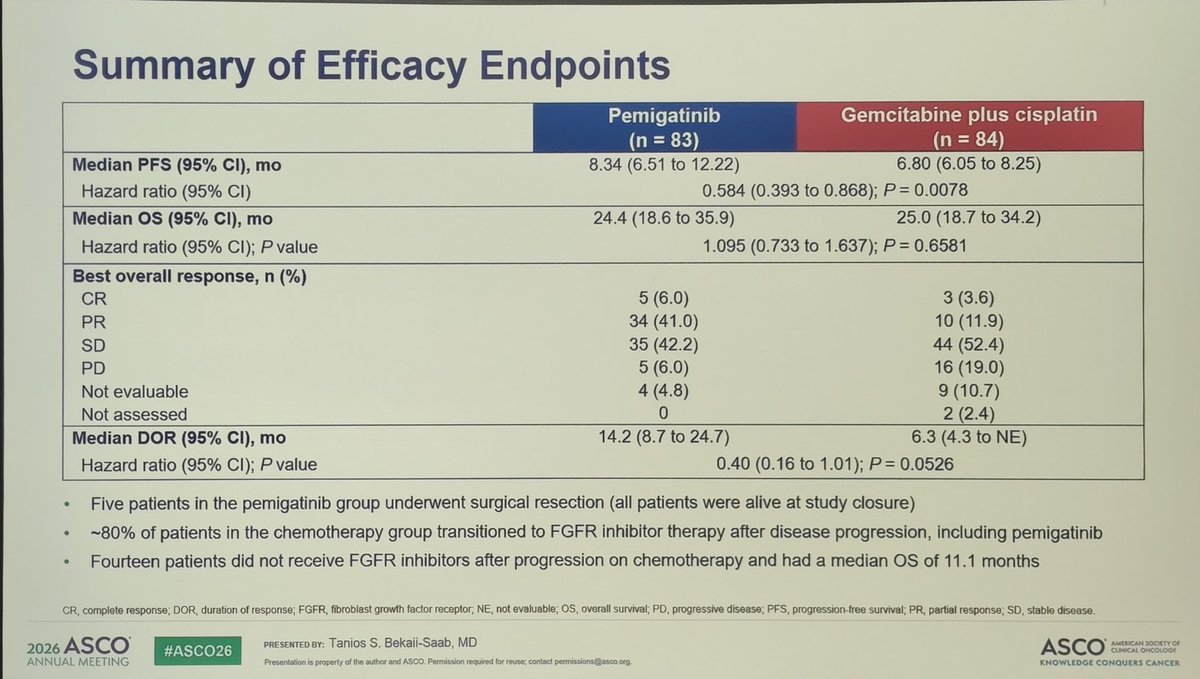
🚨 FIGHT-302 at #ASCO26
Pemigatinib vs CisGem in 1L FGFR2 rearranged BTC
• PFS 8.3 vs 6.8 mo
• ORR 47% vs 15%
• OS 24.4 vs 25 mo
🤔 Does this change the algorithm or lack of evidence given no IO + CisGem?
😯 An option for pts who need response?
@_SEOM@atuvibi@GrupoTTD
🚨 PDAC Mini-oral time at #ASCO26
Key takeaway points:
• Pembrolizumab does not add efficacy to Olaparib maintenance for gBRACA mutant PDAC.
• MEK inh + QT (modified GnP) showed promising efficacy (OS 17 mo) -> Will they play a role with KRAS inh?
@_SEOM@GrupoTTD@myESMO
Key posters on FGFR2 in BTC:
• Mut or ampl seen in ~3% of cases → eligible for targeted FGFR2inh
• Tinengotinib shows efficacy in pts pretreated with FGFR2inh
• RWD suggest FGFR2inh 1L may deliver better PFS vs CisGem+IO.
🕵️♂️ results from FIGHT-302.
@GrupoTTD#ASCO26
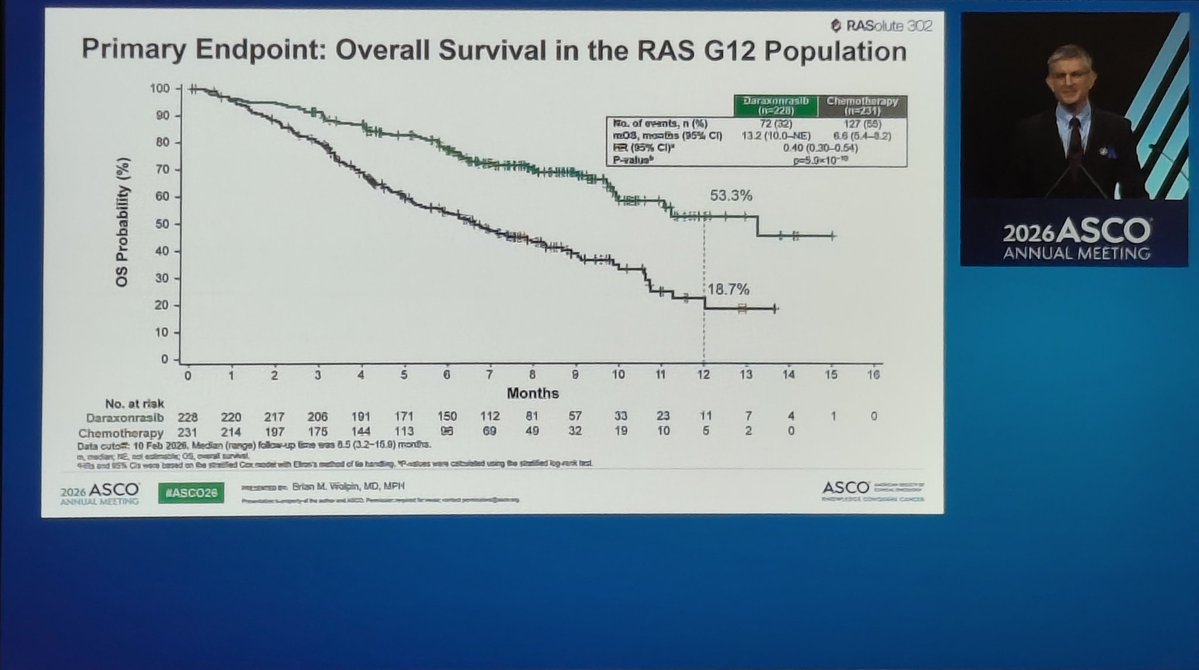
Prime time at #ASCO26 ❗ Daraxonrasib improves PFS and OS in second-line PDAC treatment compared to QT. Grateful to be part of this important moment for patients. Audience on its feet applauding, fully aware of this historic milestone.
Presented at #ASCO26:
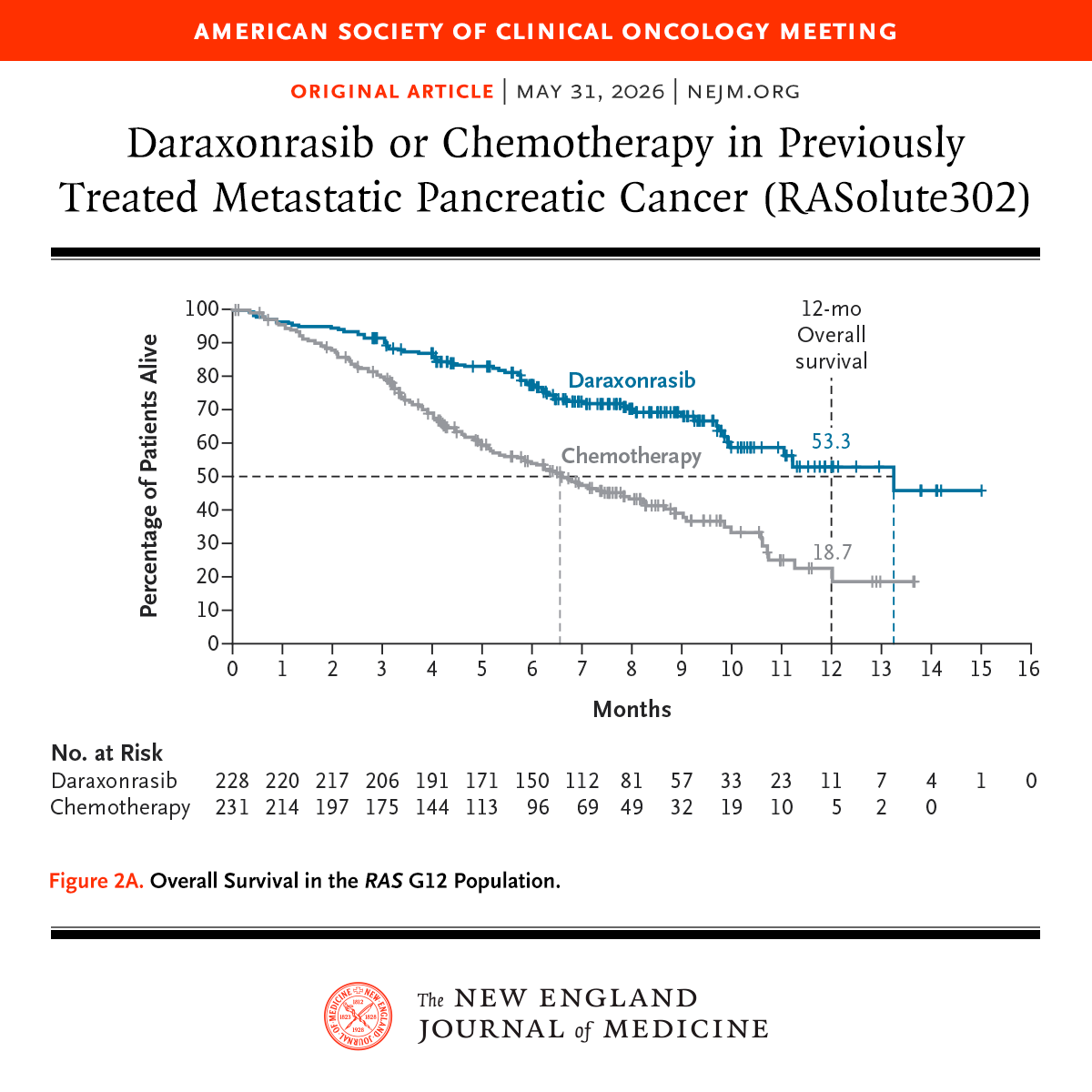
Among patients with previously treated metastatic pancreatic ductal adenocarcinoma, the RAS(ON) inhibitor daraxonrasib led to significantly longer overall survival and progression-free survival than chemotherapy. Full phase 3 RASolute 302 trial results: https://t.co/xwLWBZYRzq
@ASCO
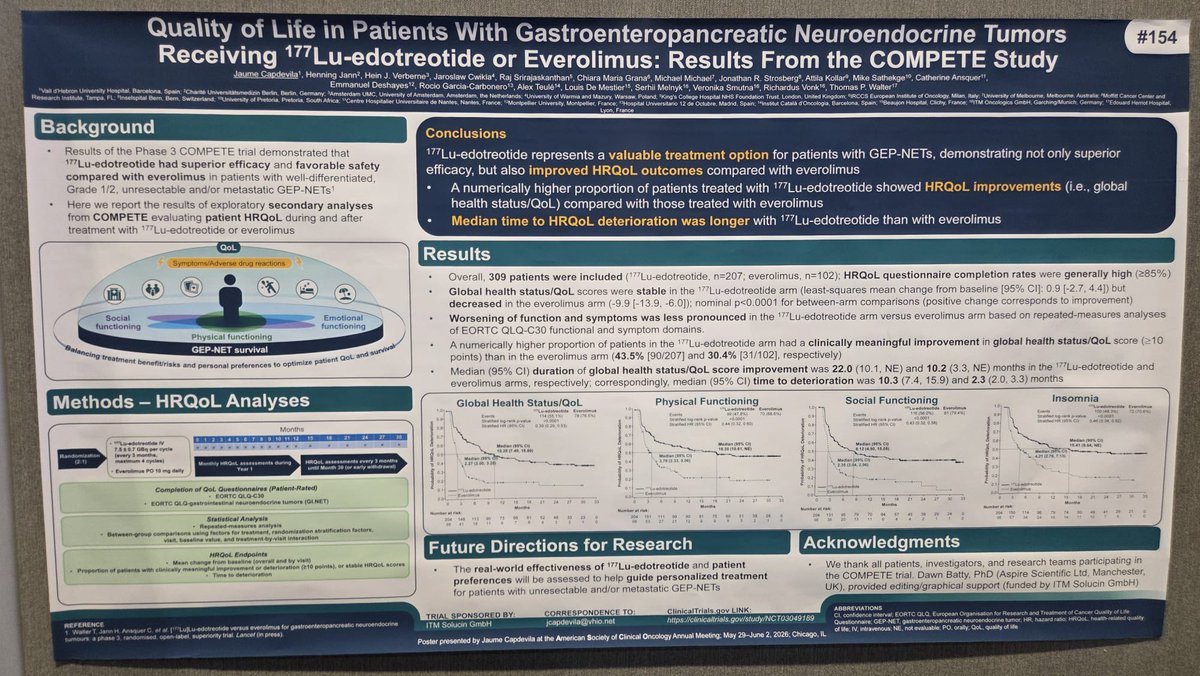
🔵 #ASCO26 | El Dr. Jaume Capdevila presenta los datos de calidad de vida del estudio COMPETE.
✔️ 177Lu-edotreotide vs everolimus
📈 Mejor HRQoL
📈 Más pacientes con mejoría clínica
📈 Mayor tiempo hasta deterioro
🎯 PRRT mejora la calidad de vida de los pacientes con TNE-GEP.
#ASCO26
This one is special.
This is the hottest paper of 2026 and potentially in the history of pancreatic cancer.
Let’s dive in.
RASolute 302: Daraxonrasib vs investigator’s choice chemotherapy in previously treated metastatic pancreatic cancer
Abstract LBA5 (soon!)
Presentation: May 31, 2026, 3:21-3:33 PM CDT
For decades, pancreatic cancer has been where good ideas go to die.
We have optimized chemotherapy. We have sequenced chemotherapy. We have celebrated modest gains.
But the central driver of PDAC has always been sitting there in plain sight:
RAS.
More than 90% of pancreatic cancers have oncogenic RAS mutations, and until recently, we had essentially nothing direct to do about it.
Daraxonrasib is an oral RAS(ON) multiselective inhibitor targeting the active GTP-bound state of mutant and wild-type RAS.
And in RASolute 302, it delivered.
Quick hits:
📌 Phase 3 international randomized trial 500 patients with previously treated mPDAC Daraxonrasib vs investigator’s choice chemotherapy
🧬 RAS G12 population
91.8% of patients had RAS G12 mutations
📈 OS in RAS G12 population
13.2 vs 6.6 months
HR 0.40
P<0.001
📈 OS in overall population
13.2 vs 6.7 months
HR 0.40
P<0.001
📊 PFS in RAS G12 population
7.3 vs 3.5 months
HR 0.45
P<0.001
📊 PFS in overall population
7.2 vs 3.6 months
HR 0.49
P<0.001
🔥 12-month OS
Overall population: 53.2% vs 17.3%
⚠️ Toxicity matters, but this was not just more efficacy for more toxicity
Grade ≥3 AEs: 61.8% vs 69.6%
TRAEs leading to discontinuation: 1.2% vs 11.2%
This is the kind of survival curve we almost never get to see in pancreatic cancer.
This validates RAS(ON) inhibition in the most RAS-addicted major cancer. It takes a target we have talked about for decades and turns it into a clinically meaningful survival benefit in a randomized phase 3 trial.
The next questions come fast: 1L combinations, maintenance, perioperative disease, sequencing, resistance, toxicity management, and whether this becomes a new backbone.
RAS is here, and it couldn’t have come sooner.
https://t.co/Y4WJRlRRTk
@TheGutonclab@UGrewalMD@TimothyJBrownMD@OncoAlert@Onco_Nexus@ASCO@NazliDizman@LauraAlderMD@DVAraujoMD@DrBarbiOnc@LauraEsfeller@FunchainMD@YGaritaonaindia@DrSAHaddad@jgong15@iandresmeraz@SakditadMD@RamilaShilpakar@RohitBanwar@lungoncdoc
The best thing about being a NETologist is that you will always find your tribe (?gang) no matter what/how big the meeting is. So good to see these amazing people at the posters session this AM. @OncoThor@Ja_Capdevila@Alej_GarciaMD#ASCO26
🇪🇸 Breaking News! Belzutifan will be made available via Spain's National Health System 🇪🇸
Congratulations to our partners in Spain for this monumental moment.
We look forward to working towards increased access to Belzutifan worldwide!
Read more: https://t.co/w1ELBRGTjY
🧠🍽️ #NUTRIGETNE (GETNE-S2109)
📌 Malnutrition in 62% of patients with GEP-NENs
📌 Sarcopenia in 15%
📌 New predictive score developed by @GrupoGetne to facilitate early nutritional screening in routine practice
💡 Simple, rapid and NET-specific tool.
🔗 https://t.co/NQtzIvWouH
🔥 A new prediction tool for malnutrition and sarcopenia in patients with neuroendocrine neoplasms, highlighting the critical role of nutrition and the power of multidisciplinary teamwork across Spain. @GrupoGetne ��🥗📊
The AGITG CONTROL NETS is finally out in paper!
Does the CAPTEM-PRRT combo perform better than CAPTEM in patients with pancreatic NETs? Well, there is more in this paper than that but let's focus on the pNETs.
Bottom line: Complex trial, many moving parts, small cohort, does not and should not change practice.
More thoughts:
The study would suggest so with longer PFS in the PRRT/CAPTEM but the bigger question is how patients who got PRRT alone compare but that was not done here. Keep also in mind that the number of treated patients was very small.
The PFS in the PRRT/CAPTEM group was 59.4 months which is very impressive (For PRRT alone reference, it was 20.7 months in OCLURANDOM and 24.5 months in COMPETE).
There were only 2 patients (3%) among those who had PRRT who developed therapy-related myeloid dysplasia which is reassuring but also goes against what others have reported where the risk is as high as 10%.
Will this change anything for me? Absolutely not as I would need larger studies to be convinced and also, I am not sure the therapy sequencing matters that much as long as you get all the effective therapy during the illness.
But what this study does is to help revive the concept of chemo-PRRT and support the development of other trials looking at combining PRRT with systemic therapy and @AmanChauhanMD, I am looking at you now... 😉
https://t.co/jY7X4snvPq