Smiley Boari flap for distal multiple strictures after multiple laser stone surgery and failed endoscopic stricture dilation, with good bladder capacity can bridge >10 cm defect easily.
Nationwide German analysis of urachal cancer (2006-2022): 2593 cases; only 530 underwent surgery. Partial cystectomy in 413, radical cystectomy in 117. Despite its aggressive nature, the majority were treated with an organ-sparing approach.
https://t.co/HclOipJ4kg
Here is a Treatment algorithm for Bone health management in patients with prostate cancer on @OpenMedicineHQ. Interactive, evidence-linked, open for discussion. Feedback welcome. #LivingAlgorithms
https://t.co/J7fMUb5ahP
@urogoldjournal publication by Joel Sheinfeld @RichMatulewicz et al:
Can Novel Biomarkers Augment Traditional Surveillance Paradigms in Early-Stage Testicular Germ Cell Tumors? Pre-Clinical Relapse Detection Using Micro-RNA-371a-3p and 372-3p Assay
https://t.co/4LV6lEyiXZ
First images from the GE Omni 128 cm Total Body PET/CT 🚀
The new scanner detected a <5 mm local recurrence of prostate cancer missed by standard PSMA PET/CT - despite 79% shorter acquisition ⏱️
Delayed imaging boosted lesion uptake and informed dose-painted salvage RT 🎯
@JournalofNucMed@PeterMacCC@declangmurphy@_ShankarSiva
https://t.co/Kiq9PHC12X
Real case: very low-risk prostate cancer (PSA 3.4 ng, Gleason 3+3, 2-12, ISUP 1) appropriate for active surveillance. A family seeks a second opinion; a surgical oncologist orders a PSMA PET-CT? and refers to medical oncology. The scan, performed at a low-experience center, is read as metastatic (bone and nodal), leading to unnecessary chemotherapy + ADT + ARPI.
When the patient returned to me, the findings did not match the clinical picture, so I recommended a second nuclear medicine review. Conclusion: rib and cervical “lesions” were inflammatory/benign uptake, not metastases. Likely technical issue: residual sodium fluoride in an aged PSMA radiotracer causing nonspecific bone uptake. No CT structural correlate.
Key takeaway: Integrate clinical context, pathology, and technical quality.
#prostatecancer
HoLEP as a cure of a metabolic problem. Interesting paper! Refractory hypernatremia in a 52yo male — BPH was the cause.
Sodium peaked at 162 mmol/L despite standard care. Diagnosis: partial urinary tract obstruction impairing renal medullary concentrating ability.
After HoLEP + cystolithotripsy: sodium normalized to 139.7 mmol/L.
https://t.co/EQK8w2SHTN
https://t.co/PSqfEB4wRN
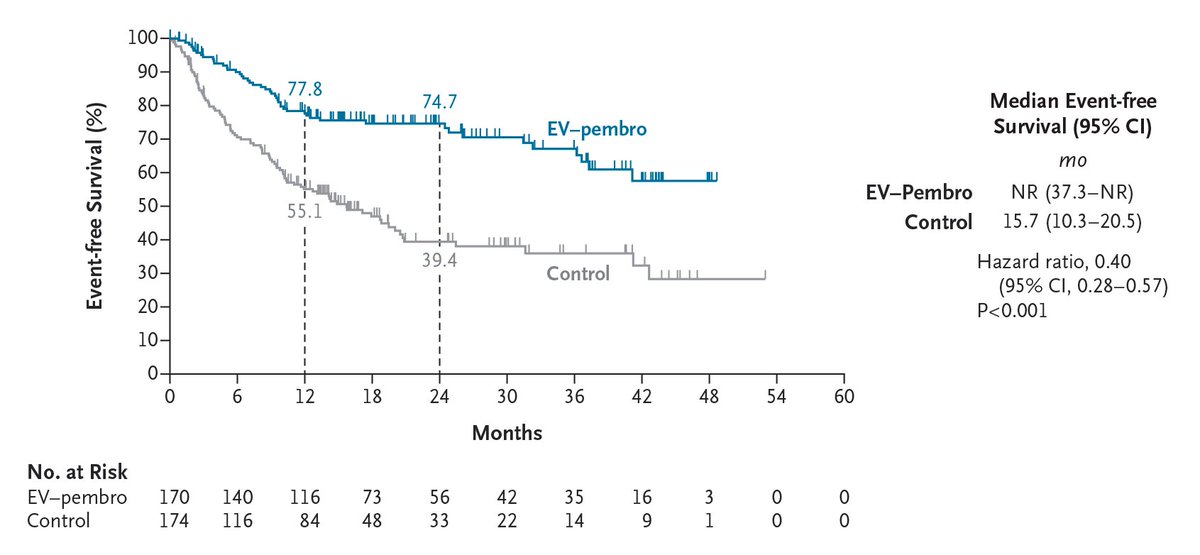
Original Article: Perioperative Enfortumab Vedotin and Pembrolizumab in Bladder Cancer (phase 3 KEYNOTE-905 trial) https://t.co/liPEVlPfHV
Editorial: Enfortumab Vedotin plus Pembrolizumab as Perioperative Therapy https://t.co/wIH8w21yJg
#Oncology
Get updated @EUplatinum published results in interactive format on our WhatsApp channel https://t.co/mcDNVdlX8e such as 👇👇 from updated pure 01 5 year data https://t.co/Co0yAFiLp4
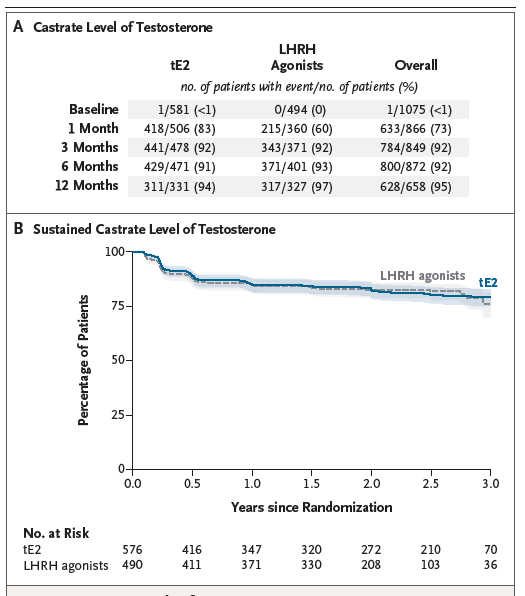
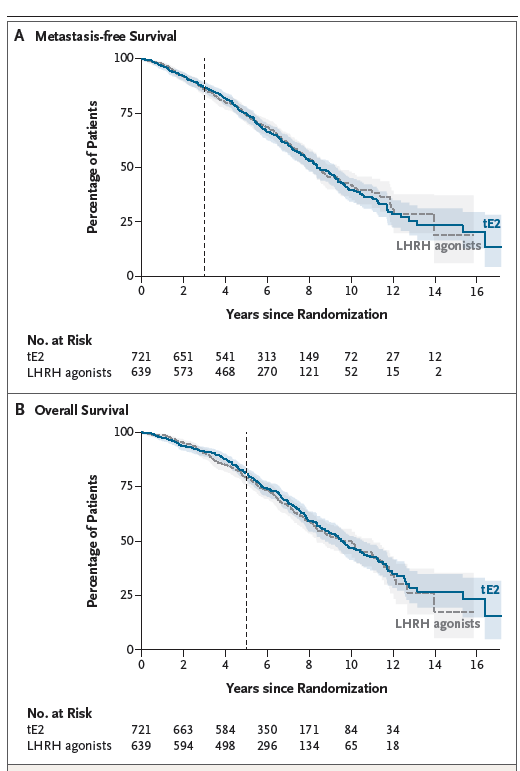
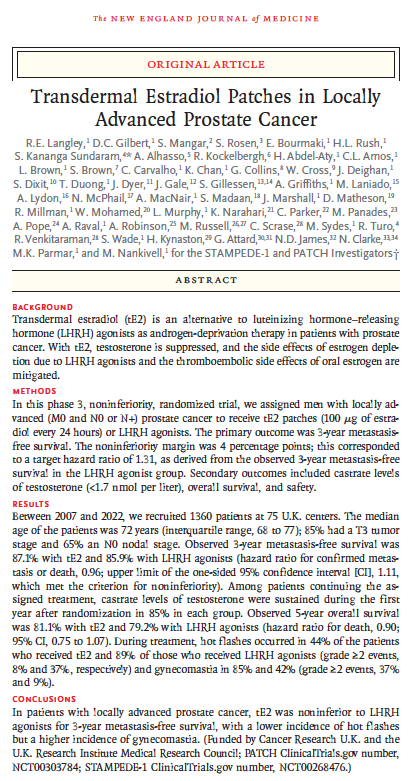
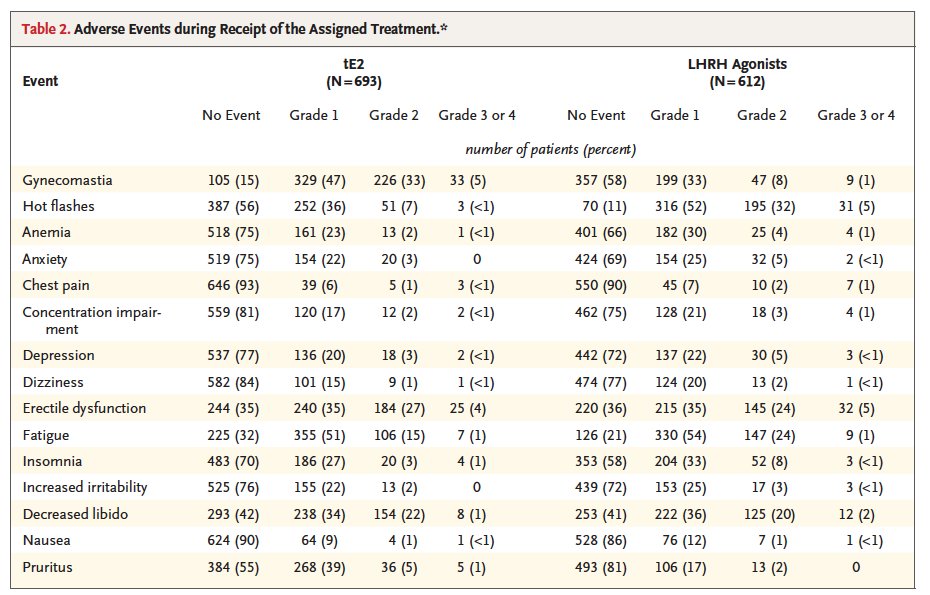
🚨Tansdermal Estradiol (tE2) vs ADT for locally advanced #prostatecancer🚨
@NEJM New phase 3 RCT (PATCH/STAMPEDE-1)
🔑tE2 patches are noninferior to LHRH agonists for metastasis-free survival (n=1,360)
✅ 87.1% vs 85.9% 3-yr MFS
🌡️ Way fewer hot flashes (44% vs 89%)
🦴 Lower fracture rates
⚠️ More gynecomastia
🔥Same cancer control. Better side effect profile. Patient-applied. Cheaper.
👀Time to rethink ADT? 👀
@PCFnews@PCF_Science@UrologyTimes@renalandurology@urotoday
🔗https://t.co/xVByp9TljJ
@tompowles1@weoncologists@Uromigos@kalasri3 Thanks for the shoutout Tom.
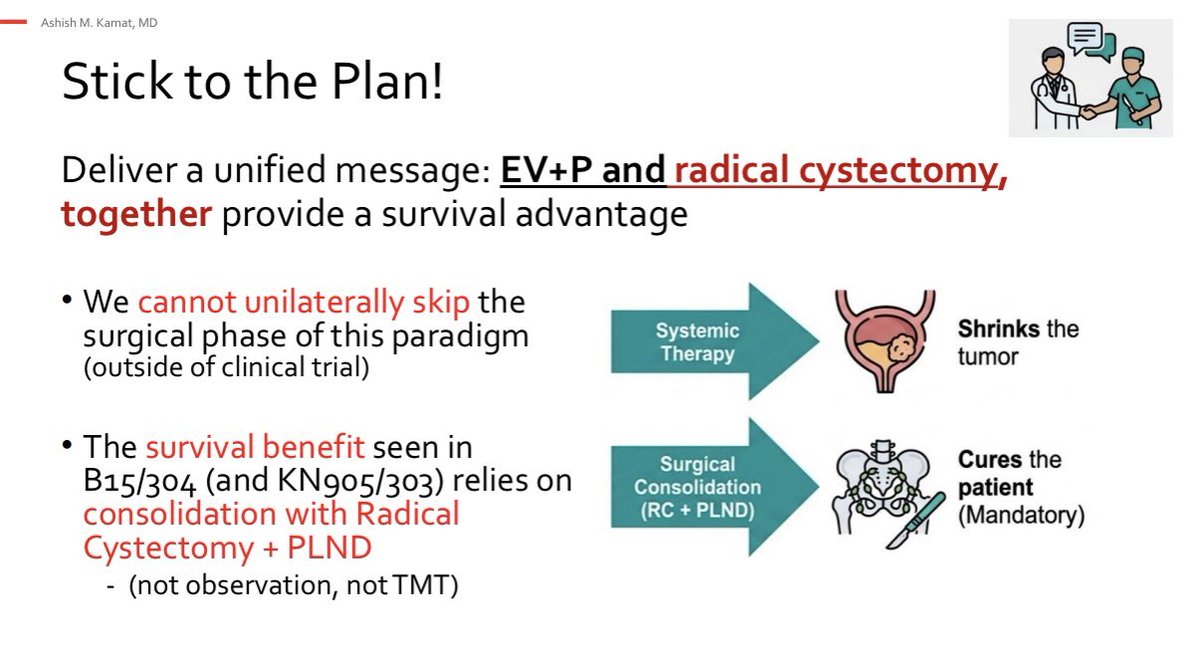
We need to help our patients and deliver a unified message:
The OS advantage seen with EV+P
relies on consolidation with Radical
Cystectomy + PLND
(not observation, not TMT)
#EAU26