Excited to share my work this upcoming week @ASCO#ASCO2026
Please come by poster board 172 - would love to connect and hear your thoughts!
Date and Time: 06/01/2026, 1:30 PM - 4:30 PM
Title: HER2-targeted tyrosine kinase inhibitors in breast cancer: Real-world analysis of gastrointestinal and musculoskeletal toxicities using the FAERS database.
Thank you @CancerExorcist for your unwavering support and mentorship!
Excited to contribute to this work exploring how AI and multi-omic signals can improve colorectal cancer screening and early detection. Important step toward more precise, population-level screening strategies. 🔬🧬 @DrArturoAI@YLeyfman@MDPIOpenAccess
Most cancers aren’t hard to treat.
They’re hard to detect early.
Our new paper proposes an AI-enabled multi-omic stool screening paradigm for colorectal cancer, integrating:
🧬 tumor DNA
🦠 microbiome
🧫 RNA
🧪 proteomic & metabolomic signals
AI can fuse these signals into precision population screening. ✨
📄 https://t.co/lk34RmQtZm
#AI #Oncology #CRC #PrecisionMedicine @mystlukes@MassiveBio@Cancers_MDPI@AmericanCancer@coloncancertask@GlobalCRC #coloncancer
Wrap up of #GI26 A memorable conference experience with impactful talks, new perspectives, and great conversations. Feeling inspired and thankful for the support and mentorship along the way. @ASCO@IMG_Oncologists@OncoDailyGI
BREAKWATER Cohort 3 at #GI26 👀
Presented by @skopetz@ASCO
Important context first. This is unlikely to be practice changing in the US, where we generally favor upfront FOLFOX. But in Europe and Canada, FOLFIRI is used upfront a meaningful amount of the time, so these data matter 🌍
BREAKWATER Cohort 3
1L BRAF V600E–mutant mCRC, n=147
FOLFIRI plus encorafenib and cetuximab vs FOLFIRI control
What we saw:
1️⃣ ORR 64% vs 39%
2️⃣ OS trend favoring EC plus FOLFIRI
HR 0.49 (95% CI 0.24 to 1.03), median OS not reached
3️⃣ Results look very consistent with what we saw in the FOLFOX cohort
4️⃣ No new safety signals
Takeaway:
Not a paradigm shift in the US, but reassuring and useful data, especially for 🇨🇦 and parts of 🇪🇺 where FOLFIRI is commonly used upfront. Always good to have more validated options for BRAF-mutant disease.
Lingering question for me:
If you start EC with FOLFIRI, do you continue EC at progression the same way many of us do after FOLFOX? Would love to see data addressing that. At least we know toxicity is ok now.
#GI26 @OncoAlert @TheGutOncLabi
Honored to have the opportunity to present our research on disparities in place of death in patients with colorectal cancer at GI ASCO 2026! Thank you @dawood_findakly for your mentorship and support #GI2026@ASCO@hemeoncfellow@oncodaily
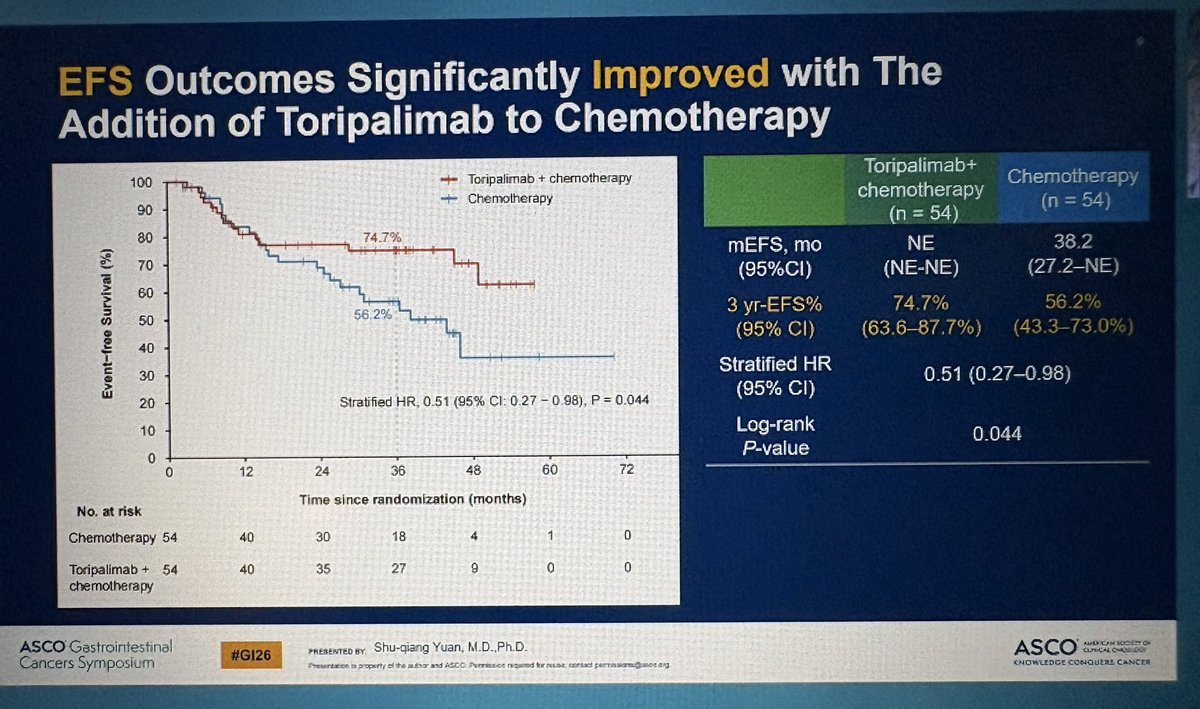
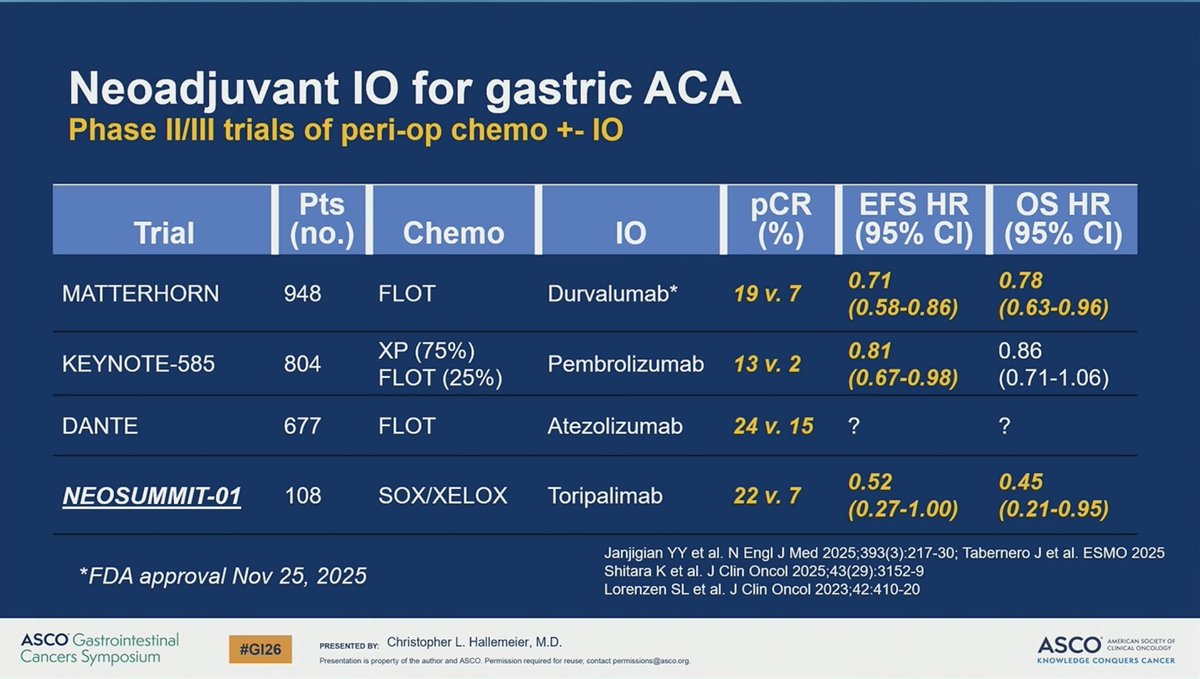
NEOSUMMIT-01 (Ph II) suggests meaningful improvement in outcomes with perioperative oxaliplatin-based chemotherapy + PD-1 inhibitor toripalimab in cT3–4N+ GC/GEJ cancers. Promising signal in a space with historically modest gains. #GI26
#GI26
NEOSUMMIT-01, now presented 🔥
Randomized Ph II perioperative oxaliplatin-based doublet (CAPEOX or SOX) ± PD-1 inhibitor toripalimab in cT3–4N+ GC/GEJC.
For context: perioperative chemotherapy alone has produced only modest gains for decades, with relapse (especially peritoneal) remaining the dominant failure pattern.
NEOSUMMIT-01 delivers something we have not seen before 👇
📈 3-year EFS 74.7% vs 56.2%, HR 0.51, P=0.044
📊 3-year OS 81.3% vs 72.2%, HR 0.45, P=0.036
🚫 Metastasis/relapse nearly cut in half: 18.5% vs 38.9%, P=0.019
⏳ mEFS not reached with perioperative chemoIO vs 38.2 months with chemo alone
Benefits held up in per-protocol analyses and after excluding dMMR patients.
🔥 The dramatic reduction in peritoneal relapse is the standout.
CAVEAT: China only study. Unclear if results will translate to a global population.
These are fantastic results and set a high bar for perioperative chemoIO in locally advanced GC/GEJC.
@OncoAlert@TheGutOncLab
KEYNOTE-937 highlights that adjuvant pembrolizumab after complete radiologic response in HCC does not improve RFS or OS, with higher ≥G3 AEs. Important negative trial shaping practice. #GI26#HCC
#GI26 KEYNOTE-937 (phase III)
🔀 Adj HCC (PEM vs PBO) after complete radiologic response (resection/ablation)
📉 RFS: 46.7 vs 45.5 mo; (HR 1.06; P=0.72)
📉 OS: 48-mo OS 79% vs 81%
🛡️ Higher grade ≥3 AEs with pembrolizumab
➡️ Adj PEM does not improve outcomes in this setting
@OncoAlert@Larvol
The evolution of KRAS inhibitors represents a major turning point in GI oncology—shifting the focus toward mutation-specific biology, resistance pathways, and strategic combinations across treatment settings. #GI26
As highlighted @asco#gi26, the development of #KRAS inhibitors underscores not only therapeutic promise, but the critical need to understand mutation-specific biology and resistance.
Trials are looking at front-line combinations, perioperative settings, maintenance strategies.
A very nice summary of the current state of evidence for neoadjuvant chemo-immunotherapy in gastric cancer by Dr. Christopher Hallemeier @MayoClinic#GI26
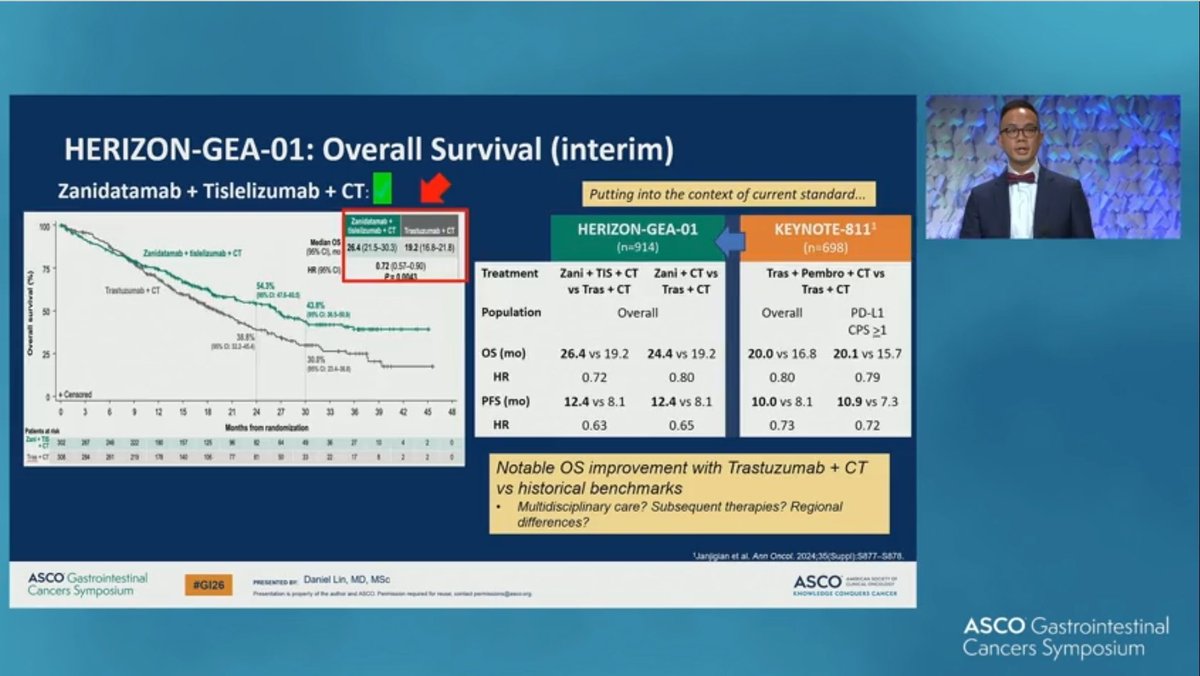
#GI26 LBA285 🔥
HORIZON-GEA-01 is presenting now.
We have a new first line.
Phase III, 1L HER2+ GEA
Zanidatamab + chemo ± tislelizumab vs trastuzumab + chemo
Key takeaways 👇
PFS significantly improved in both zanidatamab arms
OS significantly improved with zanidatamab + chemo + tislelizumab
Zanidatamab + chemo alone not significant at first interim
Cross-trial context matters.
Median OS 26.4 months here vs ~20 months in KEYNOTE-811.
Zanidatamab + chemo + tislelizumab is a new 1L standard for HER2+ GEA 🚀
@OncoAlert@TheGutOncLab
Truly honored to be a Featured Voice at the #ASCOGI Cancers Symposium. Excited to amplify important conversations in GI oncology. #GI26@ASCO@OncoDailyGI
We’re excited to announce our Featured Voices for the 2026 ASCO Gastrointestinal Cancers Symposium! Get their expert perspectives, find out which abstracts and sessions they’re most excited about, and join the conversation with the official meeting hashtag, #GI26.