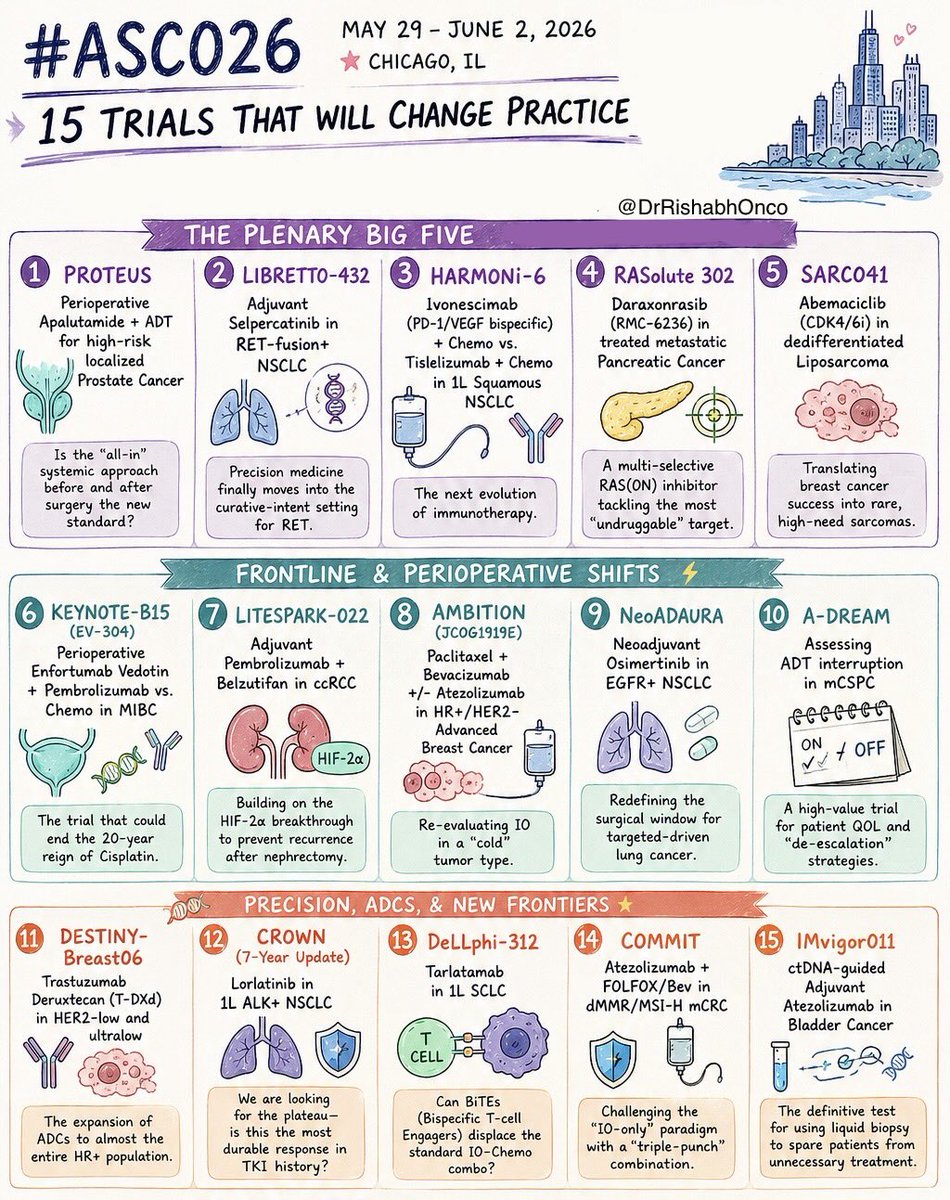
🚨 THE 15 MOST IMPORTANT TRIALS OF #ASCO26
May 29 - June 2 | Chicago
Which trial are you watching most closely?
🌟 PLENARY GAME-CHANGERS
1️⃣ PROTEUS
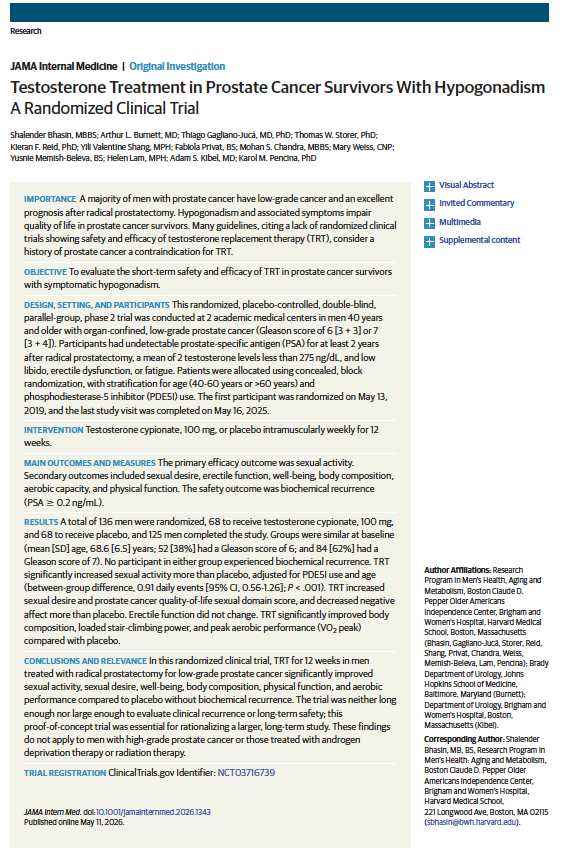
Perioperative apalutamide + ADT in high-risk localized prostate cancer
2️⃣ LIBRETTO-432
Adjuvant selpercatinib in RET+ NSCLC
3️⃣ HARMONi-6
Ivonescimab + chemo vs tislelizumab + chemo in squamous NSCLC
4️⃣ RASolute 302
Daraxonrasib (RMC-6236) in metastatic pancreatic cancer
5️⃣ SARC041
Abemaciclib in dedifferentiated liposarcoma
⚡ FRONTLINE & PERIOPERATIVE SHIFTS
6️⃣ KEYNOTE-B15 / EV-304
EV + pembrolizumab vs chemo in MIBC
7️⃣ LITESPARK-022
Pembrolizumab + belzutifan in adjuvant ccRCC
8️⃣ AMBITION
Paclitaxel/bevacizumab ± atezolizumab in HR+ breast cancer
9️⃣ NeoADAURA
Neoadjuvant osimertinib in EGFR+ NSCLC
🔟 A-DREAM
ADT interruption strategies in mCSPC
🧬 PRECISION, ADCs & NEXT-GEN IMMUNOLOGY
1️⃣1️⃣ DESTINY-Breast06
T-DXd expands into HER2-ultralow disease
1️⃣2️⃣ CROWN (7-year update)
Lorlatinib durability in ALK+ NSCLC
1️⃣3️⃣ DeLLphi-312
Tarlatamab in frontline SCLC
1️⃣4️⃣ COMMIT
Atezolizumab + FOLFOX/Bev in MSI-H mCRC
1️⃣5️⃣ IMvigor011
ctDNA-guided adjuvant atezolizumab in bladder cancer
#OncoTwitter #MedTwitter #ASCO26 #CancerResearch @OncoAlert@ASCO@JCOPO_ASCO@OncBrothers
What is the real α/β in Prostate Cancer?
In this meta-analysis in the 🟢 Journal on regard BRFS :
α/β = 1.5 → no correlation
α/β = 3 → everything changes (R² 68%)
Practical translation : we don't know the real α/β value
#radonc
🎧 Music during prostate biopsy = real clinical impact
🚨VIVALDI RCT in @EurUrolOpen
✅Patient-selected music during transperineal prostate biopsy lead to....
↓ Pain at every step (VAS consistently lower)
↓ Anxiety & distress post-procedure
↓ Sedation needs (37% vs 57%)
↑ Patient satisfaction & willingness to repeat
🫰Simple. Scalable. Zero downside.
⭐️So critical for anyone with a large Active Surveillance population
💡Nonpharmacologic interventions aren’t “soft”—they’re effective.
🔗https://t.co/0eicfj7Vxz
@PCFnews@PCF_Science@EUplatinum
[68Ga]PSMA-11 PET/CT vs. mpMRI in patients with a high suspicion of prostate cancer and previous negative biopsy: head to head, parallel, prospective trial (PROSPET-BX)
https://t.co/Ytf1goIUkH
This prospective trial compared [68Ga]PSMA-11 PET/CT and mpMRI in men with suspected #ProstateCancer after a prior negative biopsy. Among 130 patients, PET/CT demonstrated higher diagnostic accuracy for clinically significant disease than mpMRI. PSA density, PRIMARY score, SUVratio, and PI-RADS predicted significant cancer.
Investigators developed the PRIMER nomogram, which showed strong performance (AUC 0.896) for predicting clinically significant prostate cancer before repeat biopsy.
Egesta Lopci,
@FasuloVittorio@RobPeschechera@GLughezzani@OncoAlert 🚨
@silkegillessen@AOmlin@weoncologists
PEACE-2 Presented at #GU26
https://t.co/9lYVA4QnHJ
PEACE-2 evaluated whether adding upfront cabazitaxel to long-term ADT and prostate radiotherapy improves outcomes in very high-risk localized #ProstateCancer .
In this 2×2 factorial phase III trial of 761 patients, no interaction was seen with pelvic radiotherapy☢️, and cabazitaxel did NOT🚫improve clinical progression-free survival (HR 1.11), with similar overall survival across arms after a median 85 months. Toxicity was higher with cabazitaxel, and prostate cancer–related deaths were rare.
Karim Fizazi
@PaulSargos
Igor Latorzeff @AFUrologie@EnriqueGallar12@PBlanchardMD@OncoAlert 🚨
@silkegillessen@AOmlin@weoncologists
5 to 20 brain metastases.
Is whole-brain radiation still inevitable? 🧠☢️
This phase III trial challenges a long-held assumption.
🧪 Trial
Stereotactic Radiation vs Hippocampal-Avoidance WBRT
Phase III RCT | N = 196
👥 Study population
Solid tumors with 5–20 brain metastases
No prior brain RT
Median mets = 14
KPS 70–100
⚖️ Arms
🎯 Stereotactic radiation to all visible lesions
🧠 HA-WBRT (30 Gy/10 fx) + memantine
📌 Primary endpoint
Patient-reported symptom burden and daily function
(MDASI-BT over 6 months)
📊 Key result
Symptoms improved with stereotactic RT
Mean difference −1.06
Clinically meaningful
P < 0.001 ✅
🧠 Function & cognition
Better KPS and Barthel Index at multiple timepoints
Several neurocognitive tests favored stereotactic RT
None favored HA-WBRT
⏳ Survival
Median OS 8.3 vs 8.5 months
No OS difference
📉 Trade-offs
More new brain mets with stereotactic RT
Higher radiographic radionecrosis
But less steroid initiation and better QoL
🎯 Clinical takeaway
For patients with 5–20 brain metastases, stereotactic radiation improves quality of life and daily functioning compared with HA-WBRT, without compromising survival.
Precision wins when patients live with disease, not just survive it.
📖 Full paper in comment ⬇️
🔖 Save for tumor boards
#OncoTwitter #RadOnc #NeuroOncology #BrainMets
@myESMO@OncoAlert@ASCO
New in #practicalRO: Tongue-Out Radiation Therapy for Patients With Head and Neck Cancer Facilitated a Rapid Recovery From Post-Radiation Therapy Dysgeusia by Lowering Oral Tongue Dose. https://t.co/ueA0NUzRup


























![APCCC_Lugano's tweet photo. [68Ga]PSMA-11 PET/CT vs. mpMRI in patients with a high suspicion of prostate cancer and previous negative biopsy: head to head, parallel, prospective trial (PROSPET-BX)
https://t.co/Ytf1goIUkH
This prospective trial compared [68Ga]PSMA-11 PET/CT and mpMRI in men with suspected #ProstateCancer after a prior negative biopsy. Among 130 patients, PET/CT demonstrated higher diagnostic accuracy for clinically significant disease than mpMRI. PSA density, PRIMARY score, SUVratio, and PI-RADS predicted significant cancer.
Investigators developed the PRIMER nomogram, which showed strong performance (AUC 0.896) for predicting clinically significant prostate cancer before repeat biopsy.
Egesta Lopci,
@FasuloVittorio
@RobPeschechera
@GLughezzani
@OncoAlert 🚨
@silkegillessen
@AOmlin
@weoncologists](https://pbs.twimg.com/media/HCuE11FXUAA1Hrl.png)