@JNCI_Now We defined the gene expression profiles distinguishing HPV+ OPSCCs that are prone to recur after TORS-based therapy. These the tumor-intrinsic and immune-related traits were tightly interrelated and generalizeable to nonsurgical cases as well. https://t.co/YL6vpevdB4
Sharing the results of ReACT 1.0 in @NatureComms -- the first study to use HPV ctDNA to guide CRT de-escalation in higher risk HPV+ OPC. ctDNA metrics may improve risk stratification. Grateful to our coauthors. @Naveris_inc@DanaFarberNews@jdschoenfeld1
https://t.co/53tHQtj8pl
So, you want to lead a randomized trial?
I ran a poll: How many people have near veto power over the approval & design of an investigator initiated oncology randomized trial? Only 23% guessed right.
Answer: >50! @RielyMD@mtmdphd
Here are the steps to do an RCT? Thread 1/
New @Nature study: >50% of lung cancer metastases are seeded by other metastases, not the primary tumor. This "seeding from seeding" reveals a complex evolutionary cascade that allows cancer to colonize the body.
https://t.co/lYUyfRYOcP
It is a well-written editorial, and I agree with some parts and disagree with others.
However, I am very disappointed that @TheLancet would choose a member of the scientific advisory board of IBA (a proton manufacturer) to write an editorial about protons.
The author of an important commentary should not have such an intrinsic conflict of interest with the subject matter.
@weldeiry I have as yet to see an an AI tool that can mimic reasoning using basic biologic principles. Imagine if you were a student today trying to use it to understand those principles.
@LocasaleLab A misrepresentation of lO drug activity - for a few cancers, they are profoundly life prolonging and occasionally curative for otherwise incurable disease. For many other cancer types, the profound effects are limited to maybe 5pct, with another 10-30pct deriving some benefit.
📢Thoughtful discussion of the utility of #protontherapy
"[...] importance of integrating patient-reported outcomes into trial design and focusing on endpoints that matter most to long-term survivors. The goal is [...] thoughtful selection of patients"
https://t.co/Vm8G79TDB1
Come for the critically important data on protons for oropharyngeal cancer, stay for the beautifully written paper.
TORPEdO is out, and it is fascinating and instructive.
I will warn you upfront that this is a long thread, but there is a lot here to discuss!
https://t.co/zvvenb2Zpl
Background: We cure most locally advanced OPSCC patients with IMRT + cisplatin, but late dysphagia, xerostomia, dysgeusia, and weight loss still wreck QoL.
Protons spare OARs beautifully on paper. Does that actually help patients?
TORPEdO was built to answer exactly that.
Our new study on the controversial role of confirmatory HPV testing in p16+ OPCs found 6% RNAScope false negatives but no true negatives, supporting only selective, CAP guideline-based use of confirmatory tests when pre-test probability of HPV-relatedness is high. https://t.co/u5rUEFlM09
@Jdcramer has made a critical point below about KEYNOTE-689.
The EFS rules in KN-689 require careful review to interpret these results. A protocol-specific event was determined by blind independent central review (BICR), but if growth in the pre-surgical CT was perceived to be a “flare” (i.e. potential progression), surgery was supposed to proceed unless unresectable (protocol quote below). In order to be considered an event, repeat imaging was required 4-8 weeks later, and obviously if the tumor was still resectable the patient would go to surgery before then.
This definition means it was extremely difficult to have an event before surgery, even if the tumor grew and the surgery was more extensive than initially anticipated. Thus some patients may have been harmed by neoadjuvant treatment, but we would not see that in the event data.
Thus there is this important disconnect: 82 patients in the pembro arm stopped the drug due to progression (by the investigator, as shown in the CONSORT diagram), even though there were only 69 progression events (by BICR, used for endpoint analyses).
Is perioperative immunotherapy doing something favorable and important in a subset of these patients? Yes, and hopefully we can refine its use to the right population and with the right regimen (adding neoadjuvant chemo or RT?).
Is it distinctly possible/probable that some patients are progressing on neoadjuvant pembro, leading to a worse outcome in some domain, but we cannot see that in these data? Yes, unfortunately, also true.
What REALLY makes a good oncologist? in @JCO_ASCO
After 10 years and 203 JCO essays, one thing became clear: expertise alone isn’t enough.
Patient-centered care.
Clear, authentic communication.
Emotional intelligence.
And the harder work
Showing up again and again.
Openness to uncertainty.
Carrying the burden of cancer care.
Continuous growth.
Clinical competence is expected
Human connection makes the difference.
Science treats disease.
Presence treats fear.
https://t.co/g9hGjSLpGu @OncoAlert
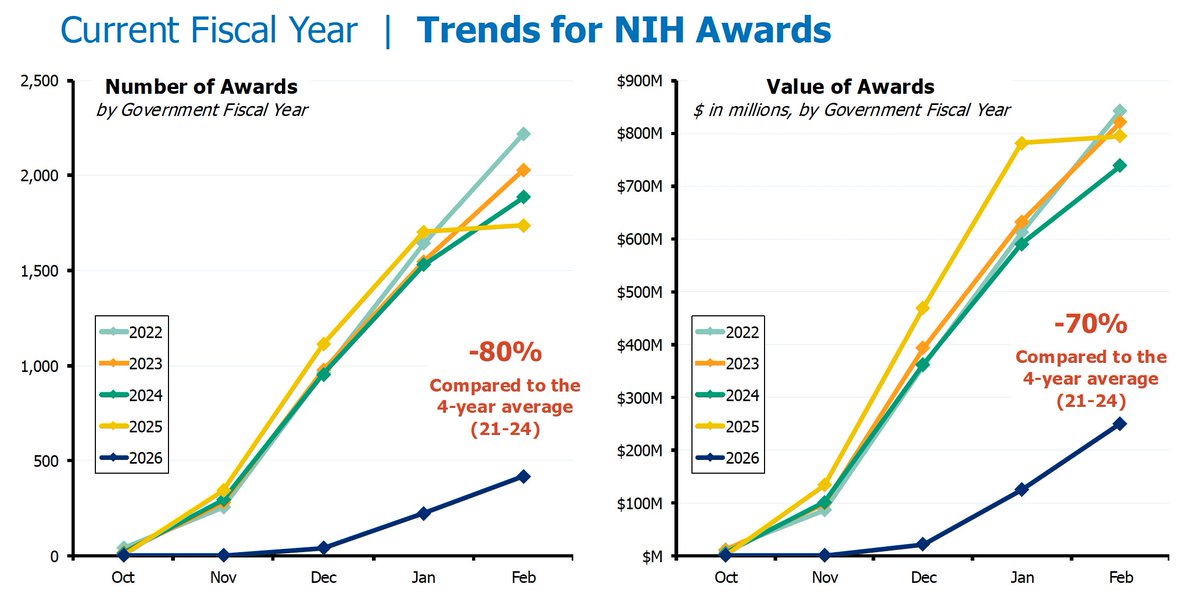
Federal funding for US biomedical research is moribund.
Since October 1 2025, NIH is -80% in new grants and -70% in values (total dollars).
Labs are closing down and researchers are leaving science.
To what end?
It was a privilege to present today at the 9th annual DDR Summit in Boston , representing the @PennCancer
team advancing translational science and clinical trials for HPV+ head and neck cancer @DiabLabPenn@DrNickLukens@LovaSunMD
Two papers in @NatureCancer highlighting the role of intratumoral bacteria & associated immune architecture (e.g., neutrophil influx) in mediating resistance to immunotherapy in head & neck cancer.
https://t.co/wrq9btzS0l
https://t.co/g5AaHgWJ09
@GeneCollector@xrtGenomics