Join us tomorrow (9/9/24) from 7-8:30 PM for an overview and case-based discussion of the WADL approach to VT ablation.
Link to register: https://t.co/eNqIS0bgAc
@BIDMC_VT@davilandre, @syang_md, Andy Locke, @BidmcCvi@JNJMedTech#ablateVT
@MDTolgaAksu Prayers for all those devastated by the earthquakes... What a great way to rally support - nothing better than tuning into EP for a good cause!
Dear Colleagues
As you know that Türkiye has recently been struck by devastating earthquakes. 10 cities have been severely affected. In this difficult time, to ask for your support, we organize an online EP meeting to discuss novel and advanced EP techniques with leading experts
6 years ago on this day we lost Mark Josephson. Mark’s life and career were extraordinarily. A giant and one of the founders of clinical electrophysiology, his numerous contributions remain as relevant today as they have been originally, and his book remains the bible of EP.
@udaysandhu8@forkknifecab_EP@masonmaps Our approach: "Term"=first site: AFL slowed/terminated late in lesion. Extended into SVC to cover "upper isthmus" and snuck down into "lower isthmus" (pacing before each burn). Did not go to IVC as ?prior scar/block. Final CS pace map suggest fixed block. Noninducible after.
Last case as fellow for @udaysandhu8... Prior CABG, persAF, arrived in typical AFL. Term with CTI, during PVI went into AF➡️atypical AFL. LAT/Voltage, EGMs, and sites of phrenic capture (green=intermittent). Best ablation strategy? #EPeeps@forkknifecab_EP@masonmaps
This is a masterpiece tweetorial that reviews many concepts and techniques for complex lead extraction. I may be biased, as I'd do *exactly* the same things as sequentially described here. Every darn step.👍
Lead extraction is an amazing area where we learn so much from others!
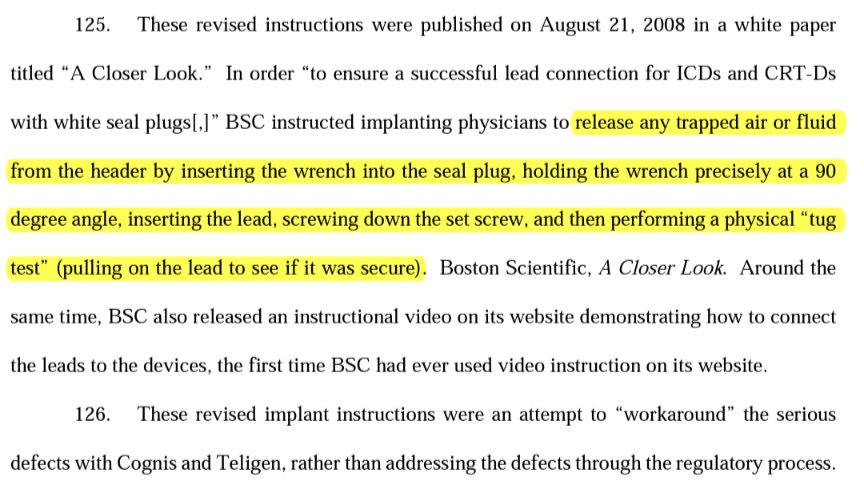
@narrowQRS@jeffrey_vinocur We had a case of this during my fellowship and were told we must not have inserted the wrench before inserting the lead into the port, to break the seal and allow air to escape. Did a google search and found this from a lawsuit against BSC in 2017!
First isolated the RPVs and post wall to clean up the substrate (good tip from @Davilandre) which made interpreting the induced flutter straightforward! Terminated with first abl then anchored to prior lines. Noninducible after! @forkknifecab_EP#HDGrid#EPeeps
Sharing a great case from last week: prior cryoPVI, roof, and CTI lines, with recurrent atypical flutter (but presented in sinus). RIPV/carina connected, as well as slowing and fractionation in the post wall and anterosept wall...