TRB does it again! inaugural release of 2023 Dorsey Detert Vineyard Cabernet Sauvignon! Dark, inky, brooding, nose of violets and mocha, velvety, silky full bodied with an endless finish! Wine of the year for me! #wine
Without treatment, 2-year mortality in HFrEF is 35%. With all 4 evidence-based therapies? 9.5%. 🧵
📉 Cumulative impact of GDMT on 2-year mortality:
❌ None — 35.0%
💊 + ARNI — 25.2% (↓28%)
💊 + Beta Blocker — 16.4% (↓35%)
💊 + Aldosterone Ant. — 11.5% (↓30%)
💊 + SGLT2i — 9.5% (↓17%)
Total: 72.9% relative risk reduction | 25.5% absolute risk reduction | NNT = 4
Treating just 4 patients with full GDMT saves 1 life over 2 years. That’s among the most powerful NNTs in all of medicine.
And all 4 drugs are now available as generics for ~$420/year. The evidence and the access are both there.
#HeartFailure #HFrEF #GDMT #CardioTwitter #EvidenceBasedMedicine #NNT
@gcfmd@SJGreene_md@AndrewJSauer@mvaduganathan@safchat@GianluSava@BiykemB@JavedButler1@ankeetbhatt@hfcollaboratory
Cardiometabolic disease does not fit neatly into silos, and our care models should not either.
I am proud that Saint Luke’s Mid America Heart Institute is part of the new CHROME initiative, a national multisite effort launched with the AMCP Research Institute to evaluate how comprehensive cardiometabolic care models work in the real world, including their clinical impact, operational structure, patient and provider experience, and economic value.
This is exactly the kind of work the field needs.
We already know that many evidence-based therapies can improve outcomes in obesity, diabetes, cardiovascular disease, kidney disease, and related conditions. The harder question is how to organize care so the right patients are identified earlier, treatment is started more effectively, multidisciplinary care is sustained, and health systems and payers can realistically support it at scale. CHROME is designed to help answer those questions.
At Saint Luke’s Mid America Heart Institute, through the Michael & Marlys Haverty Cardiometabolic Center of Excellence, we have been committed to building and studying practical care models that improve diagnosis, treatment uptake, and long-term outcomes. Our participation in CHROME reflects that mission and gives us an opportunity to help shape the evidence base for what modern cardiometabolic care should look like.
What makes this initiative especially important is that it goes beyond clinical endpoints alone. CHROME will also examine governance, staffing, referral pathways, treatment protocols, diagnostic workflows, patient experience, provider workflows, payer decision-making, and implementation barriers.
That is where scalable care models either succeed or fail.
I am grateful to partner with AMCP Research Institute, Lilly, Geisinger, and the Patient Advocate Foundation’s Patient Insight Institute on this effort. If we want to close the gap between evidence and execution in cardiometabolic care, this is the kind of work that matters.
https://t.co/tH9aAp2u0g
Summary of all Late-Breaking Trials at #ACC2026 – take home points
@ACCinTouch@ACCmediacenter@JACCJournals
1. HI-PEITHO: Ultrasound-facilitated catheter-directed thrombolysis led to a lower risk of PE-related death, cardiopulmonary decompensation or collapse, or recurrence of PE. vs anticoagulation alone in intermediate-high risk PE.
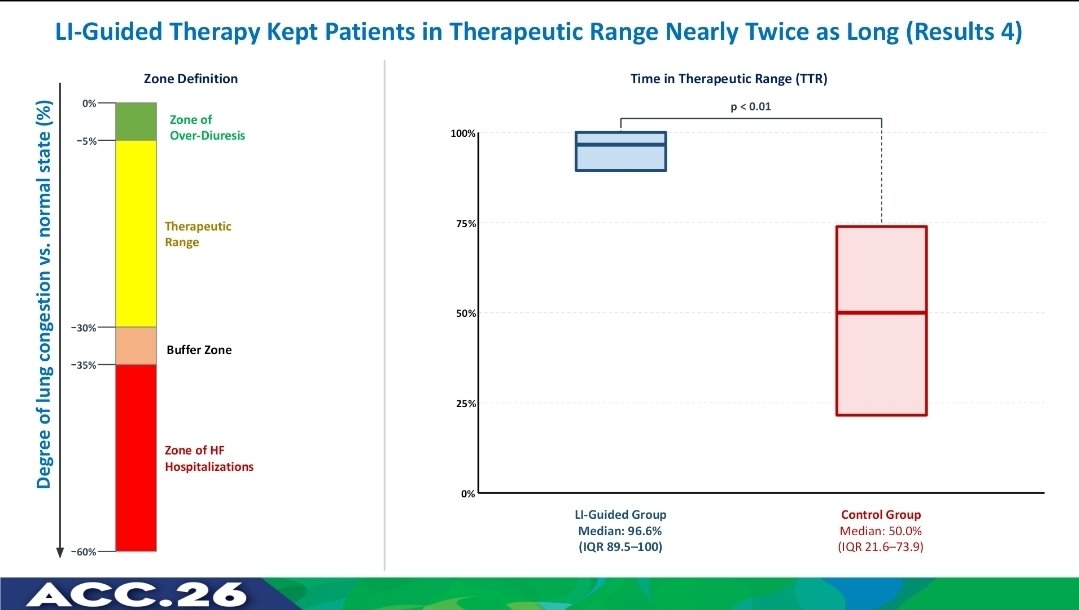
🚨 IMPEDANCE-HFpEF — #ACC26
One of the most anticipated trials delivers striking results
🔑 Noninvasive lung fluid monitoring:
• ↓ 81% HF hospitalizations
• ↓ 65% all-cause mortality
• Earlier and more frequent treatment adjustments
🧠 Detecting congestion before symptoms may change how we manage HFpEF
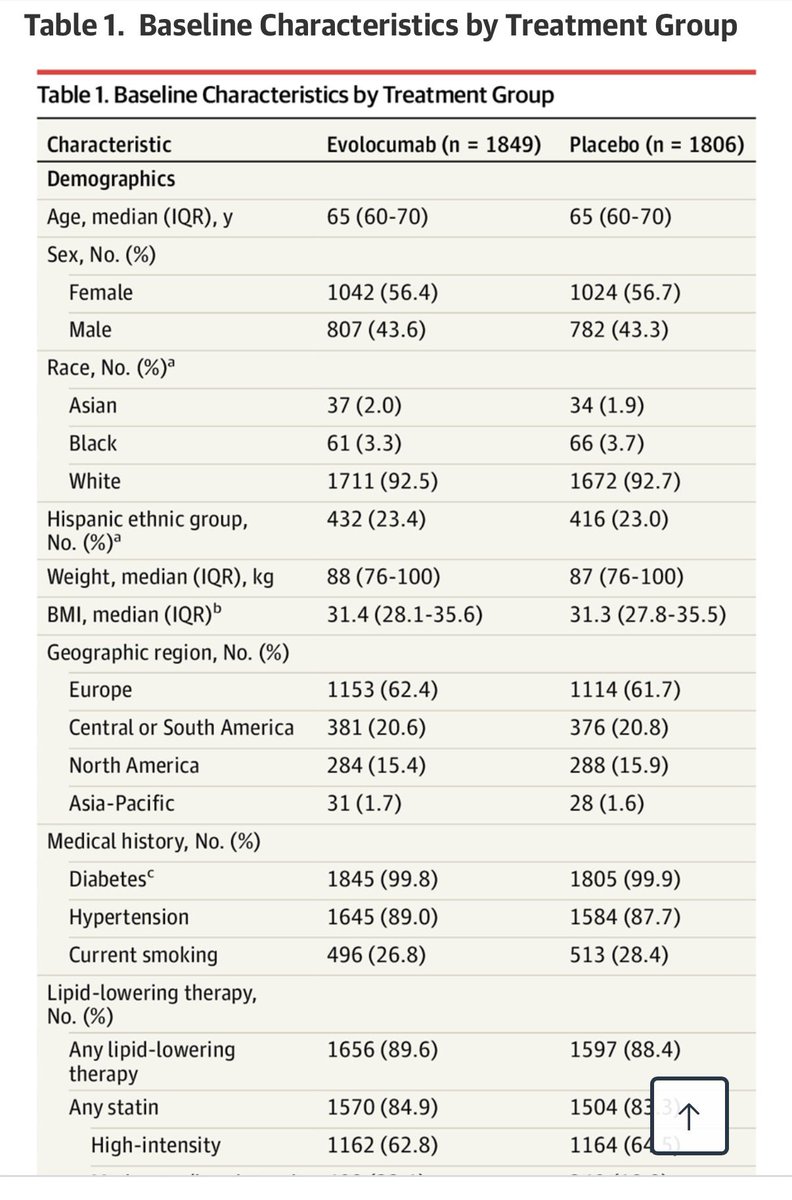
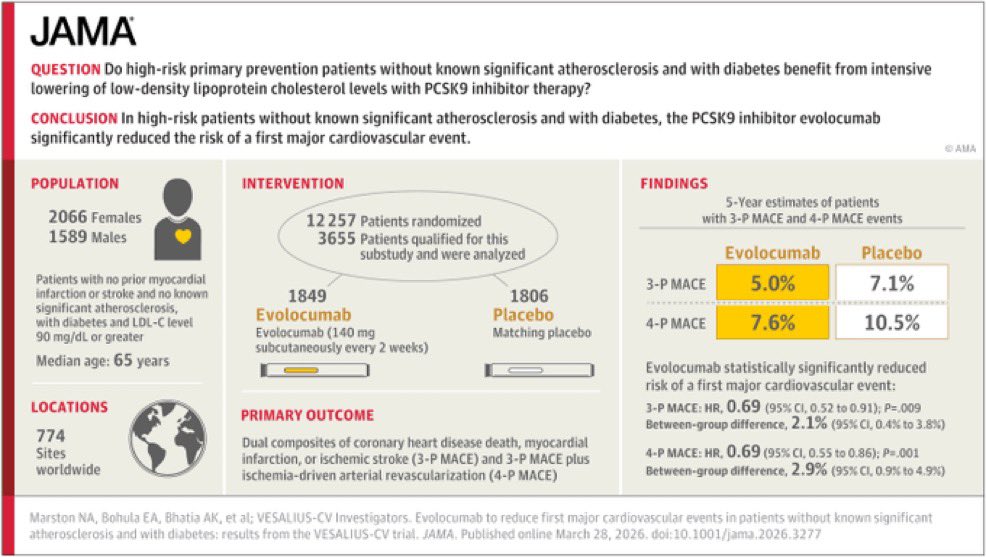
PCSK9 inhibitors transformed secondary prevention—
but what about primary prevention?
#VESALIUS-CV evaluates evolocumab in patients without established ASCVD.
Could this expand who we treat—and when?
➡️ Key results: evolocumab⤵️ CV events in this high risk primary prevention study!
56% 💃🏻
92% White
#ACC26 #Lipids #CvPrev @JAMACardio
📎 https://t.co/CP1BMKI45X
@jwalkermobile Rough starts, but finish strong! Competition is getting tougher by the round. We’ve got a team that can win it all, but all top seeds are stronger than I can ever remember! Go devils!!!
An important addition to the literature. Interestingly- and let me know if you see things differently- this should not change the practice among those who were already following the @AHAScience@ACCinTouch@HRSonline guidelines: if an AF patient at risk for stroke truly cannot safely tolerate long-term anticoagulation, it remains reasonable (as a 2A recommendation) to place one of these devices. Also, more based on anecdote and common sense, those with a prior LAA clot, particularly if found while on a #DOAC, may still benefit from placement of an LAA occlusion device AND continuation of an anticoagulant. There really never was adequate evidence to support large scale use of these devices as straight-up substitutes for DOACs.
@DrJMarine@UCSF@UCSFCardiology@UCSFHospitals@drjohnm@ethanjweiss@DrDave01@DrRoderickTung@JonPicciniSr
A 102-year-old woman who had been married for 78 years was asked on her deathbed what she wished she had done differently.
Her answer made her 80-year-old daughter weep.
Here is what she said…