@AJWLight@thetimes misleading headline or at the very least open to misinterpretation from general public reading this piece which doesn't do anyone any favours
Just read the new Light et al. focal therapy paper in European Urology. In short: beyond fatally flawed marketing brochure with a DOI. Here's the autopsy 🧵
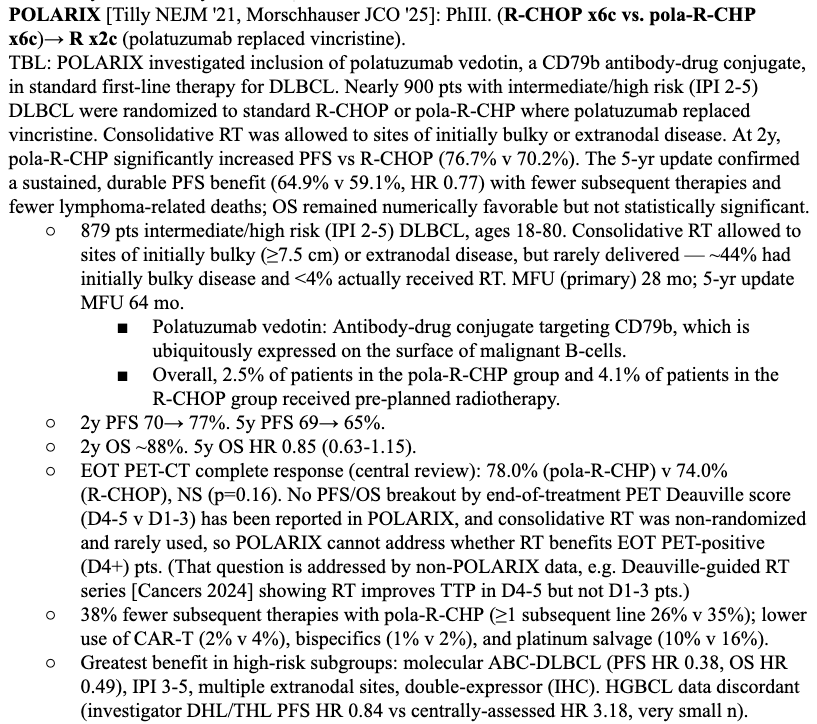
1/ As with POLARIX, the end-of-treatment PET non-CR subgroup went unreported in POLARGO. We still haven't seen Deauville 4+ EOT outcomes for POLARIX, where ~22% were D4+, yet the low ~3% RT utilization rate was touted as a victory without PFS shown within the D4+ subgroup(!)
Definitive Radiotherapy to the Primary Tumor in Stage IV NSCLC: A Consensus Statement From the International Association for the Study of Lung Cancer Advanced Radiation Technology Subcommittee - Journal of Thoracic Oncology https://t.co/TcXhgMqRts
In a retrospective cohort of 68 DLBCL patients with partial metabolic response on interim PET after 4 cycles of R-CHOP, PET-directed residual site RT was associated with improved response and PFS.
29 patients received additional R-CHOP + risk-adapted pRSRT:
• Deauville 4: 24 Gy
• Deauville 5: 40 Gy
Compared with no RT, pRSRT improved EOT CR:
• Overall: 72.4% vs 41.0%
• Deauville 5 subgroup: 83.3% vs 22.2%
PFS also favored pRSRT:
• 2-year PFS: 85.8% vs 52.9%
• 5-year PFS: 57.2% vs 44.1%
• Multivariable HR 0.26, p=0.018
No statistically significant OS difference was observed, with limited events and no deaths in the RT cohort. Toxicity was generally manageable, though one grade 4 bowel perforation occurred.
Although this cohort was treated in the R-CHOP era, the question remains highly relevant in the POLARIX/pola-R-CHP era: when residual PET-avid disease persists despite improved systemic therapy, PET-directed RT may still have a role as a selective consolidation strategy. #lymsm #DLBCL #OncTwitter
PROTEUS - paper says BCF is <0.2. Supplement and some talk here shows it was moved to <0.02 for time to biochemical failure. 0.02 isn't in the article. Anyone have insight?
Obviously the lower you push this, the more the event free curves will separate with intensification.
@CanesDavid@DrSpratticus PSMA isn’t very reliable with only 40% sensitivity for nodal metastases
PSA is the best marker to trigger for additional salvage curative local therapy but the reliability of PSA is lost with perioperative ADT
My vote is still RP alone with risk stratified treatment thereafter
Interesting read! All radical treatments for pca have toxicities. The key issue for pts is not simply if toxicity occurs, but which toxicities persist and how they affect long-term QOL. Transient GU symptoms are not equivalent to permanent incontinence or impotence
1/ 🚨 New @NEJM: Perioperative enfortumab vedotin + pembrolizumab (EV+pembro) in MIBC (KEYNOTE-905)
Congrats to the authors on an important randomized phase 3 trial in a tough, cisplatin-ineligible population 👏
Let’s walk through it 👇
#GU26 and #fengsymposium was a blast to see progress.
Hoping it eventually moves away from San Fran 😁. Another red eye on the books back home.
My observations from PCa sessions:
- the field continues to push for over tx and many fail to recognize high risk dz is not high risk anymore for most patients. Enzarad negative, Rtog 0924 neg, ascend-RT neg for MFS/OS, peace2 neg. RT+ADT plenty for most. Many need even less. Select trials paving the way.
- for mHSPC not all patients need doublet let alone triplet; age matters
- continuous ADT can often be more harmful than helpful now with MDT
-most BCR patients post RP do not need ADT—> get biomarker testing to help
-many have jumped on bandwagon that OS too hard to improve and settling for early non-surrogate endpoints; peace3 should remind us it’s possible
-sequential PARPi /Abi often just as good as combination
-early germline/somatic testing for all high risk disease remains without data to support it; even testing in mHSPC unclear benefit as can give PARPi in mCRPC setting (earlier not better than later).
-actinium RLT promising but toxicity remains concern
-neoadj before RP remains largely ineffective, adds costs and toxicity and most still need postop tx.
A reminder that if a British broadcaster accused a political party of “shamelessly pandering to Jews” they’d be out of a job. But, hey ho, it’s open season on Muslims in the British media. Again.
Wow, that Cochrane review on nurse vs doctors is actually REMARKABLY bad. So, it's obviously an interesting question, and I was totally suprised to see there have been 19 RCTs comparing mortality between nurses and doctors (!). And the reported CI is tight RR 1.03 (0.87 to 1.21)+
In a first-of-its-kind meta-analysis, an MD Anderson study found metastasis-directed therapy significantly improved outcomes in patients with oligometastatic prostate cancer.
Read more: https://t.co/oNIMcfzIFi @ChadTangMD#EndCancer