I noticed an analogy between how some friends of mine are working, in a little apartment above a bakery, and how Anthropic engineers seem to be working, in a great big building with a bakery in it, and I noticed some similarities. No. Not the bakery. Why would you think that.
https://t.co/cgsuofJNdZ
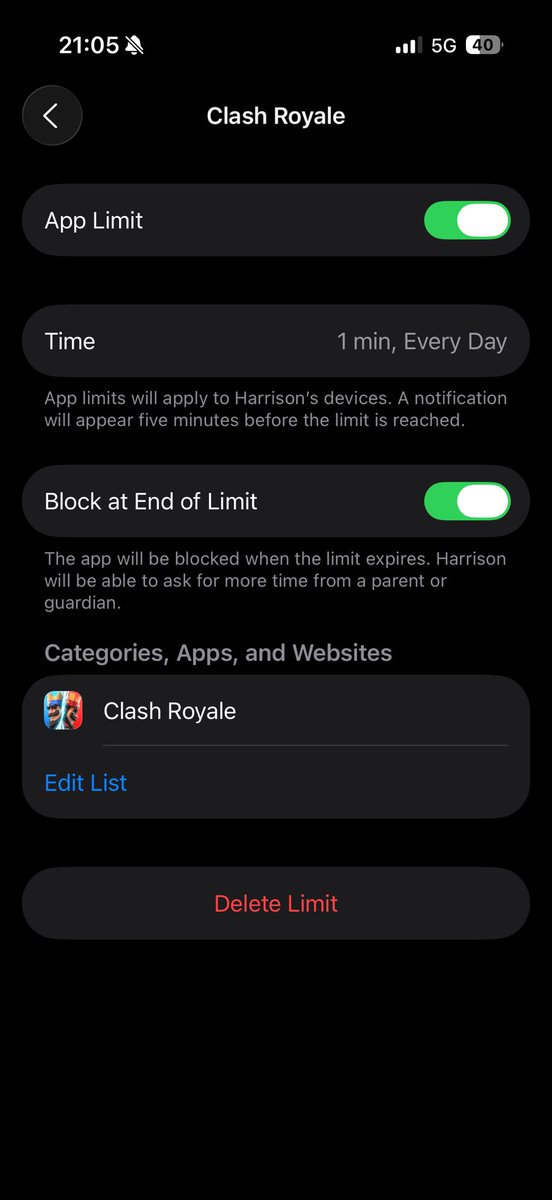
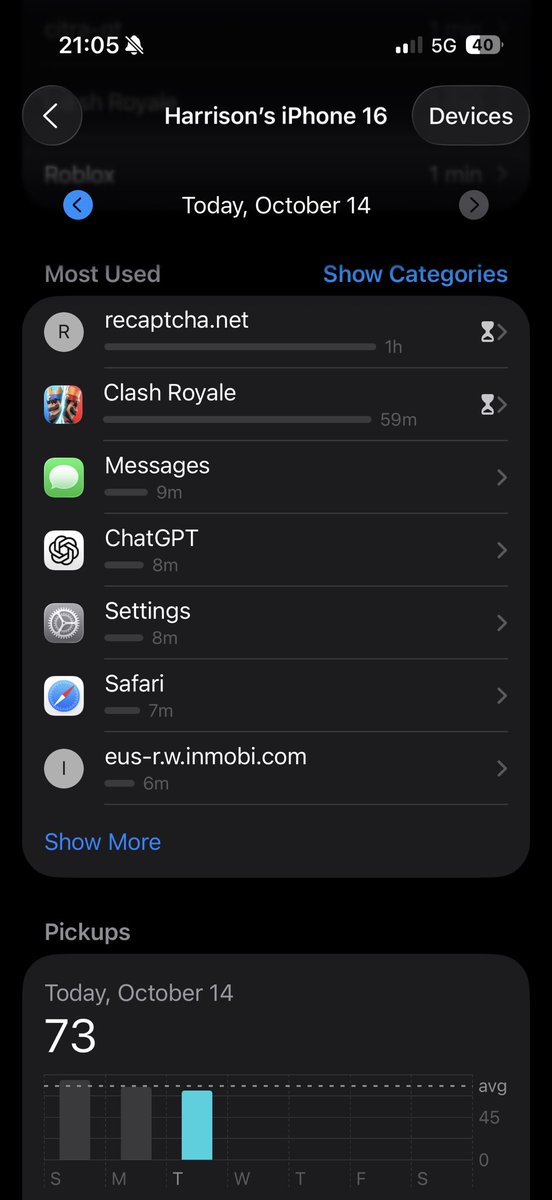
Paging anyone at Apple to fix the steaming pile of garbage that is Apple Screentime. The whole team should be fired. It never works, WSJ and others report on it, Apple never fixes it. Below from my son today.
@JoannaStern
I just want to emphasize: This is not normal. This is unprecedented. And it is chaos.
This morning my colleagues -- who are working quite hard -- reported that the White House had decimated CDC offices related to injury prevention, respiratory disease surveillance, and chronic disease, as well of all the staff that edit the CDC's MMWR, one of the most important medical journals.
Now *some* of those cuts are being walked back, but HHS won't even speak on the record.
I have been a reporter who has covered health care and medicine for 20 years and this does not match with anything I remember seeing.
Read more from @cooney_liz, @ChelseaCirruzzo, and @HelenBranswell.
https://t.co/TYZVK3BZGE
One of the most promising areas for the application of AI in medicine is scaling specialty expertise. There simply aren't enough specialist doctors to care for everyone in need. We believe AI can help.
As a first step towards that goal, we worked with the amazing Google medical AI team to tune and test their conversational agent AMIE in the setting of Stanford's Center for Inherited Cardiovascular Disease.
Unlike many medical studies of LLMs, we completed our testing not with curated cases or exam questions but real-world medical data presented in exactly the way we receive it in clinic.
Data was in the form of reports derived from multi-modal data sources including medical records, ecgs, stress tests, imaging tests, and genomic data. AMIE was augmented by web search and self-critique capabilities and used chain-of-reasoning strategies fine-tuned on data from just 9 typical patients.
What did we find?
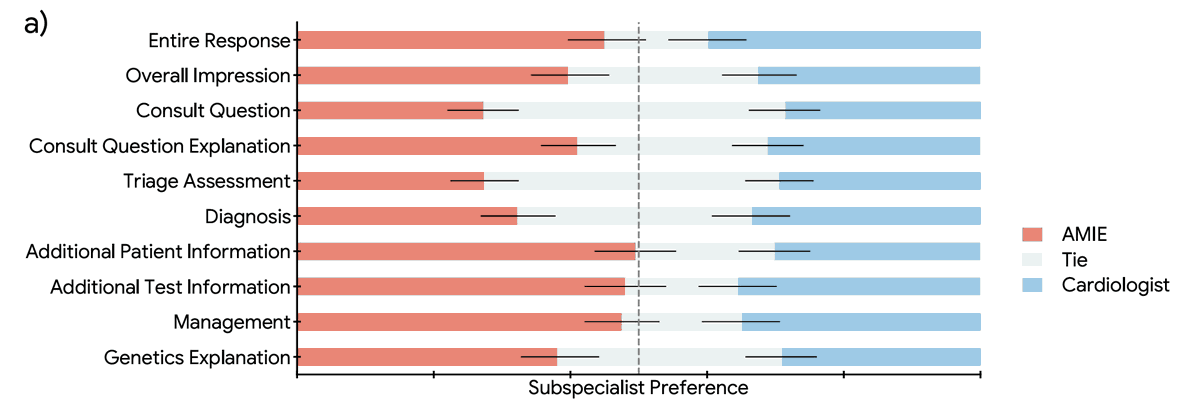
1. Overall, AMIE responses on diagnosis, triage and management were rated by specialty cardiologists as equivalent to or better than those of general cardiologists across 10 domains.
2. Access to AMIE's responses improved the general cardiologists' responses in almost two thirds of cases.
3. Qualitative data suggested that the AI and human approaches were highly complementary with AMIE judged thorough and sensitive and general cardiologists judged concise and specific.
In conclusion, our data suggest that LLMs such as AMIE could usefully democratize subspecialty medical expertise augmenting general cardiologists' assessments of inherited cardiovascular disease patients.
Paper: https://t.co/NsA2pcOS6Y
Generative podcast describing the paper (!): https://t.co/qSDpEXEgsZ
Stanford Center for Inherited Cardiovascular Disease: https://t.co/YvgN1YM90X
AMIE: https://t.co/fN1V1UFdWY
Congrats to @DrJackOSullivan and @taotu831 for leading the charge on this work as well as the @StanfordDeptMed team and the amazing folks @Google led by @alan_karthi and @vivnat
Difficult categorical clinical decision: who to see first, who gets transplant, watchful waiting for cancer or treat aggressively: myriad preferences that inform decision. No single gold standard decision exists because preferences are as varied as life stories of humans. I have a brief blog post https://t.co/B7PkGGPwV2 to introduce a study (https://t.co/NbJ3QzVIVM) of how frontier LLM align themselves with diverse gold standards and how well they can be aligned. I also introduce a simple measure, the Alignment Compliance Index.
This study was inspired by this review we published @NEJM https://t.co/kBlLoo9jTE with @kunhsingyu@Liz_Healey_@arjunmanrai and Tze-Yun Leong https://t.co/Hx16bkVhI0 and discussions in lab meeting with Noa Dagan @ClalitResearch & @MattBMcDermott
Comments are welcome.
📢 Super excited to share our new study @NatureMedicine on developing and validating an explainable graph-based foundation model for drug repurposing, designed specially for rare diseases, which collectively affect 300 million patients globally!
🧵1/10
People ask me all the time for AI use cases in healthcare
So last month, we hosted the first OOP hackathon using generative AI tools
Here are all the projects that were made in 36 hours. They made me more optimistic about the future
Exciting news! 🎉 Introducing the Open Medical Reasoning Tasks project!
Inspired by @NousResearch and @teknium, @OpenLifeSciAI ( Open Life-Science AI ) is launching an open, collaborative initiative to create a comprehensive list of medical reasoning tasks for LLMs! 🧠🏥
To all physicians, researchers, data scientists, and visionaries pioneering the fusion of AI and healthcare: This is your call to action! The future of medicine needs your expertise. 🦸♀️🩺🧠🦸♂️
🔬 Contribute to advancing AI in healthcare
🤝 Join a community of medical professionals & AI researchers
📚 Build better training datasets & benchmarks for medical AI
Explore and contribute on GitHub: https://t.co/YsMP2tIR3P
Open Source AI Is the Path Forward!! Let's revolutionize medical AI together! 🚀 #OpenMedicalAI #AIinHealthcare #Medical #Clinical #healthcare #ai #chatgpt #health #llms
I'm starting a company, Datalab:
- Task-specific models that outperform frontier LLMs and existing tools
- Examples: my projects marker and surya (25k GH stars) with task-specific arch
- Goal: Train models, open source as much as possible, do hosted inference and on-prem
I just released new surya layout and text detection models:
- 30% faster on GPU, 4x faster on CPU, 12x faster on MPS
- Accuracy very slightly better
- When I merge this into marker, it will be 15% faster on GPU, 3x on CPU, 7x on MPS
Listening to Leo Celi's state of the dark arts in real world deployments now at #CHIL2024 -- lots of great content, and a great reminder to this paper https://t.co/JTXkQE2xcj by @TravisZack2, @Emily_Alsentzer, et al -- fantastic exploration of how LLMs may exacerbate biases
MS4 here publishing something on this soon. the clinician stack is changing quickly...
the aforementioned plus:
- @AbridgeHQ - SOAP notes, discharge & patient summaries, etc.
- @AtroposHealth - real world evidence studies to address specific clinical questions underserved by literature
- @ChatGPTapp@AnthropicAI literature summaries, pathophys explanations, memory aids, etc.
- @ambossmed@uworld content / board prep
- @mdcalc clinical calculators
- @SketchyLearning micro + pharm, simulation
Brilliant lecture by Mark Thomas on using AI to select antithrombotic therapy. International guidelines recommend 17 drugs for treatment of ACS in different settings. This means there are over 50 million possible treatment combinations. #ISTH2024
Some challenges in building LLM-powered applications (including RAG systems) for large companies:
1. Hallucinations are very damaging to the brand. It only takes one for people to lose faith in the tool completely. Contrary to popular belief, RAG doesn't fix hallucinations.
2. Chunking a knowledge base is not straightforward. This leads to poor context retrieval, which leads to bad answers from a model powering a RAG system.
3. As information changes, you also need to change your chunks and embeddings. Depending on the complexity of the information, this can become a nightmare.
4. Models are black boxes. We only have access to modify their inputs (prompts), but it's hard to determine cause-effect when troubleshooting (e.g., Why is "Produce concise answers" working better than "Reply in short sentences"?)
5. Prompts are too brittle. Every new version of a model can cause your previous prompts to stop working. Unfortunately, you don't know why or how to fix them (see #4 above.)
6. It is not yet clear how to reliably evaluate production systems.
7. Costs and latency are still significant issues. The best models out there cost a lot of money and are very slow. Cheap and fast models have very limited applicability.
8. There are not enough qualified people to deal with these issues. I cannot highlight this problem enough.
You may encounter one or more of these problems in a project at once.
Depending on your requirements, some of these issues may be showstoppers (hallucinating direction instructions for a robot) or simple nuances (support agent hallucinating an incorrect product description.)
There's still a lot of work to do until these systems mature to a point where they are viable for most use cases.
🚀 Exciting News! 🚀
We're thrilled to announce that our longitudinal electronic health record (EHR) dataset, EHRSHOT, is now available for download! 🌟
📊 6,738 patients
📅 41.7M events
🩺 921,499 visits
Details at: https://t.co/g3TDVBEJsv
Nice, a serious contender to @lmsysorg in evaluating LLMs has entered the chat.
LLM evals are improving, but not so long ago their state was very bleak, with qualitative experience very often disagreeing with quantitative rankings.
This is because good evals are very difficult to build - at Tesla I probably spent 1/3 of my time on data, 1/3 on evals, and 1/3 on everything else. They have to be comprehensive, representative, of high quality, and measure gradient signal (i.e. not too easy, not too hard), and there are a lot of details to think through and get right before your qualitative and quantitative assessments line up. My goto pointer for some of the fun subtleties is probably the Open LLM Leaderboard MMLU writeup: https://t.co/Ns1hfEct4k
The other non-obvious part is that any open (non-private) test dataset inevitably leak into training sets. This is something people strongly intuitively suspect, and also why this GSM1k made rounds recently
https://t.co/0jzJNb2SXK
Even if LLM developers do their best, preventing test sets from seeping into training sets (and answers getting memorized) is difficult. Sure, you can do your best to filter out exact matches. You can also filter out approximate matches with n-gram overlaps or so. But how do you filter out synthetic data re-writes, or related online discussions about the data? Once we start routinely training multi-modal models, how do you filter out images/screenshots of the data? How do you prevent developers from e.g. vector embedding the test sets, and specifically targeting training to data that has high alignment (in the embedding space) with the test sets?
And the last component of this is that not all LLM tasks we care about are automatically evaluateable (e.g. think summarization, etc), and at that point you want to involve humans. And when you do, how do you control for all the variables involved, e.g. how much people pay attention to the actual answer, or the length, or the style, or how refusals are treated, etc.
Anyway, good evals are unintuitively difficult, highly work-intensive, but quite important, so I'm happy to see more organizations join the effort to do it well.