A crucial task in psychiatry is to clarify a distinction that is rarely overt: 🚨distinguish between a patient seeking symptom relief vs a patient seeking change. ( or both)
Relief involves the reduction of distress and restoration of stability.
Change often requires modification of maintaining patterns, which may transiently increase distress.
The therapeutic process becomes challenging when the clinician mistakes the desire for relief as readiness for change OR when the patient expects change without the discomfort that often accompanies it.
🚨Weekend 7 hr GP Mental Health Skills Training in Melbourne. Here are 5 Principles of Psychiatric Assessment for GPs that I use as a foundation 👇
1. Time is a therapeutic intervention
Psychiatric assessment is iterative and needs time before the pattern and the understanding behind the pattern becomes clearer.
Change also needs time. The brain ‘resists’ change when it’s spent significant effort organising around a certain state.
2. Diagnosis is a process, not a label
A diagnosis is not about labelling.
The diagnostic process involves:
Diagnostic hierarchy → formulation → diagnostic construct
The label is useful, but it is only one part of understanding the person’s presentation.
3. Start with phenomenology
Begin by clarifying the patient’s lived experience: what they feel, perceive, think, fear, avoid, repeat, or cannot do.
Symptoms have to be converted to phenomenology.
I am feeling anxious # anxiety
It may be agitation
Phenomenology can be mapped through PACES:
Perception – Activity – Cognition – Emotion ( Hedonics) – Sleep
4. Evaluate the range of factors contributing to the phenomenology
Once the phenomenology is clear, evaluate the possible contributing factors:
biological, psychological, social, developmental, cultural , diet and life style related factors.
‘The question is: What are the dominant facts and what are the points of
attack for modification and adjustments?’ (Meyer, 1951)
The task is to understand why this pattern of distress has emerged in this person, at this time.
5. Let formulation guide STAGED management
Management follows from the formulation.
The aim is symptom relief / control and a return to meaningful functioning, as defined and made visible by the patient.
Psychiatric management is staged, iterative and based on hypothesis testing: treat, observe, revise the formulation, and adjust the plan.
Here is a list of things to practice/work on (in sequence of which you should focus on) to become a “good enough” beginner-ish therapist. IMO. FWIW. It’s all stuff we continue to refine and master over years, but you can get the hang of it enough to be “good enough” first. 1/
Incredibly grateful to David Ross for the opportunity to collaborate, NNCI, our producer Robert Scaramuccia, all our guests, and the mentors, colleagues, friends, and family who helped make this possible.
I wrote more about the backstory here:
https://t.co/7RHBkMLBHf
New from NNCI’s Ten to the Fifteenth: a 7-part podcast series on brain stimulation in psychiatry.
~7 minutes each, covering ECT, TMS, DBS, and emerging treatments, with interviews from leaders in the field.
Available on all major platforms
https://t.co/Hi2KjSoQnU
One of the best parts was getting to learn from leaders across the field, including @NoahSPhilipMD, @SarahLisanbyMD, @Martijn_Figee_, Andy Leuchter, and Nolan Williams.
The season covers history, mechanisms, clinical use, and future directions in neuromodulation.
I’d say that driving forces behind these large scale trends are societal forces, constraints and incentives of clinical practice, investor interests and agendas, and collective professional self-interest. The academic class interested in recognizing and commenting on these trends usually has very limited ability to do anything about it. When there is high consumer demand, alternatives are limited, treatments are imperfect, and clinicians are limited in their ability to provide thoughtful, relational, informed care, overprescription and iatrogenic harm are basically inevitable.
New publication! 🧠
Excited to share our latest paper, for which I am co-first author. This randomized controlled trial provides the first evidence that #buprenorphine can prolong and augment #ketamine’s antisuicidal effects in depression.
https://t.co/kxDE7cdg2R
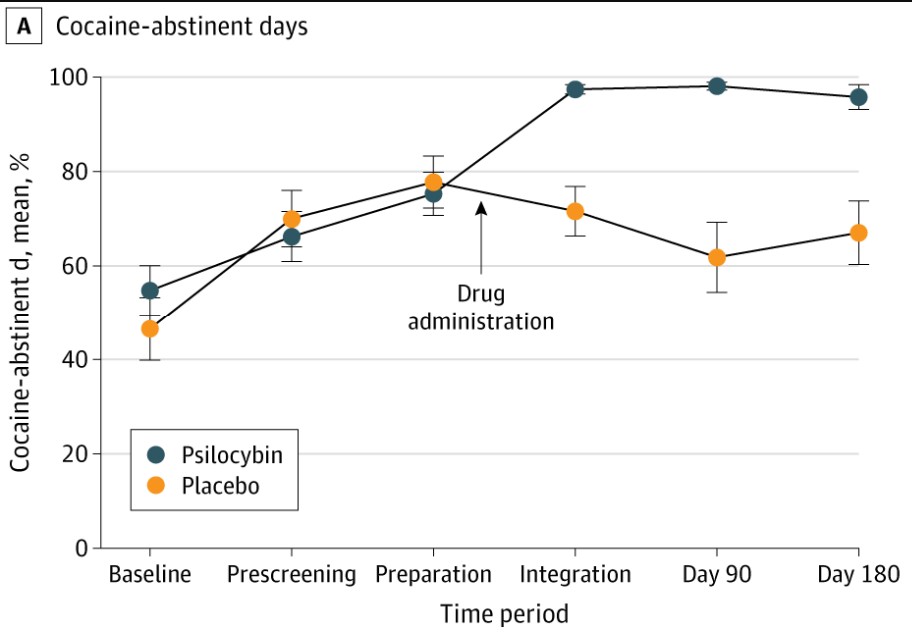
For 50 years the National Institute on Drug Abuse has spent hundreds of millions of dollars to find an effective cocaine addiction medication. After 100+ molecules & many hundreds of studies nothing has been FDA approved. It's the Holy Grail of addictions medication. Proud to have helped Peter Hendricks & team at UAB in a trial showing psilocybin to treat cocaine addiction.
🚨🍄 Major new preprint alert 🍄🚨
I think these will be important results. They are not going make me popular with my #psychedelic in-group, please do not shoot the messenger!
The premise of this pre-registered meta analysis (https://t.co/qEvCE9u31B) is that it is biased to compare open-label trials to blind trials, it is only fair to compare open-label trials to other open-label trials. In the first case the open-label trials would gain an unfair advantage by benefitting from effects related to knowing the treatment. Therefore, we compared the efficacy of psychedelic-assisted therapy (PAT), which is open-label regardless of formal blinding to open-label traditional antidepressants (tAD; such as SSRIs/SNRIs where binded trials are very close to be truly blind) for the treatment of major depression.
We tested 3 prior hypothesis (MCID: minimum clinically important difference, which we set to be 3-points on Hamilton depression scale; differences smaller than this are clinically meaningless):
1. At the primary endpoint, the estimated mean difference between PAT and open-label tAD will exceed the MCID, favoring PAT.
2. At the primary endpoint, the estimated mean difference between blinded and open-label tAD trials will exceed the MCID, favoring open-label administration.
3. At the primary endpoint, the estimated mean difference between blinded and open-label PAT trials will not exceed the MCID.
In contrast with our prior hypothesis, we did not find PAT to be more effective than open-label tADs (H1). Not only was the difference not clinically meaningful, but practically there was no difference at all (~0.3 HAMD units). This finding means that tAD administered knowingly to patients, which is the case in real-life medical practice, is as effective as PAT. This result was robust across variations in study selection, including when we removed PAT trials on treatment-resistant depression. The improvement from baseline to endpoint was ~12 HAMD points for both treatments.
We also assessed the impact of blinding in both PAT and tAD trials. We found that for tAD (H2), but not for PAT (H3), open label is associated with better outcomes than blinded treatment. However, even in the case of tAD, the difference was much lower than the MCID.
How come hypothesis 1 failed, i.e. that PAT is no ore effective than open-label tADs, given that tAD trials are famous for small drug-placebo difference (~2.4 HAMD units), while PAT trials reported large effects (~7.3 large effects)? Well, there are two major factors:
1. As we show, open-label tAD is approximately ~1.2 HAMD units more effective than blinded treatment (H2). This effect can be interpreted as the influence of knowing one’s treatment assignment, such as positive expectancy.
2. A recent meta-analysis of depression trials found that relative to tAD trials, the placebo response is 4.0 HAMD points lower in psychedelic trials (Hsu et al., 2024). This suppressed placebo response leads to an inflated between-arm difference, as the treatment arm is measured against a lower floor.
The sum of these two effects is 1.2 + 4.0 = 5.2 HAMD units which equals the difference of the reported between-arm effects (7.3 - 2.4 ~ 5), explaining why hypothesis 1 failed.
The suppressed placebo response in PAT trials is likely attributable to the ‘know-cebo’ effect, i.e. the disappointment when patients realize they are in the control group. In PAT trials, this placebo suppression accounts for 4.0 / 7.3 ~ 55% of the total between-arm effect. In other words, ~55% of PAT’s between-arm effect is not explained by improvement in the treatment arm, but rather by the lack of improvement in the placebo arm.
In summary, we found that for the treatment of depression, PAT is no more effective than open-label SSRIs/SNRIs. Our results for psychedelics are twofold: PAT demonstrated a robust and large therapeutic effects (~12 HAMD units), which justifies optimism. On the other hand, PAT’s lack of superiority compared to SSRIs/SNRIs under equal-unblinding conditions highlights the influence of blinding integrity and presents a sobering reality check for psychedelic medicine.
In collaboration with @QuantPsychiatry and Hannah Barnett 🙏🫂
👆should be of interest to @MattBurkeMD@igoreckert@bita137@Brainclinics@bruce_lambert@thelablab@IoanaA_Cristea@GregFonzo@MFPL6@fredemag@n_sepeda@chchatham@LGHemkens@HolBjo@NaudetFlorian@NathanHuneke@RecoveryDoctor@iainjordan@GlynLewis9@HengartnerMP@shayla__love@f_hieronymus@And_Cipriani@FlamelingJop@JD_Rosenblat@RickZeifman@AVoineskos@LukeJelen@TehseenNoorani@a_lisinski @PloederlM @ElliotMarseille@KingFranklinIV @JulesEvans11 @EikoFried@ExistWell@singletonion@_fernando_rosas@vincepsy@hartogsohn@MichielElk@JacobSAday@BWe1ss@sdpnayak@Colloca_Luana@JeremyHowick@mattbagg@TheBorisLab@BenColagiuri
Come do a Psychedelic MSc (!) with us, ON CAMPUS, @UniofExeter, with amazing interdisciplinary lecturers, a lively research community, access to beautiful nature, and a lot of passion for magical substances.
https://t.co/22wMPTFukW
This extraordinary psychedelic precision functional mapping dataset is now fully/freely available to all!
All the info to access & use it in a newly published Nature Scientific Data Resource: https://t.co/W6lRzv7u2b
Thanks to the incredible team who created it - Subha S, Rick R, Ginger N, Demetrius P, Nick M, to name a few.
New in @NatureMedicine: ReSPCT "An international Delphi consensus for reporting of setting in psychedelic clinical trials" by @ChloePronovostM, Kyle Greenway, myself, and many ReSPCT Experts. "The ReSPCT guidelines and accompanying explanatory document provide a new standard for the design and documentation of extra-pharmacological variables in psychedelic clinical research."
https://t.co/wNnggwG0z9
https://t.co/7YeQXsbsTe
Major praise to the @nyulangone podcast team.
I expected just a little internal thing, but they did an AMAZING job digging into the science and creating a great show.
Check it out -
YouTube (full-length): https://t.co/MgqRrs7cvY
Podcasts: https://t.co/WLNVni4UaE
Spotify: https://t.co/5L6TIXOh50