Top Tweets for #scienceSaturday

👩🏫📖✨This #ScienceSaturday, every teacher brings a unique story into the classroom. This study examines how one science teacher's life history informs her views of science and the way she teaches it. #TeacherEducation #EducationResearch 💡Read here: https://t.co/90pXXcs5NA

🧬 #ScienceSaturday
❓Could what we eat influence how well cancer immunotherapy works?
Researchers have long observed an “obesity paradox” in cancer care: although obesity is linked to many health risks, some patients with a higher body mass index appear to respond better to immune checkpoint inhibitors. A new study explored whether body weight itself is responsible, or whether diet and the gut microbiome may offer a better explanation.
➡️ Researchers tested 12 different diets in mouse models treated with anti-PD-1 therapy. They found that treatment response was more closely associated with the animals’ diet and gut bacteria than with body weight, body fat or other measures of metabolic health.
➡️ Some diets created a gut environment that supported a stronger immune response against tumors. These dietary changes altered the types of bacteria living in the gut and the substances, or metabolites, those bacteria produced.
➡️ One bacterium that stood out was Lactobacillus johnsonii. On its own, the bacterium modestly improved the response to immunotherapy. A supportive diet also helped. But when the bacterium and diet were combined, they produced a much stronger response than either did alone.
➡️ The researchers also identified a bacterial metabolite called desaminotyrosine, or DAT, that appeared to help activate tumor-fighting T cells. These immune cells produced stronger signals and became better equipped to attack cancer after anti-PD-1 treatment.
➡️ Interestingly, changing the animals’ diets could reshape the microbiome and influence treatment response within days, before major changes in weight occurred. This suggests the benefit may come from how food affects gut bacteria, rather than from obesity itself.
➡️ The team also transferred gut bacteria from human patients into mice. Even microbiota from a patient who had not responded to immunotherapy could support a better response when paired with a favorable diet, showing how strongly diet may shape the activity of the microbiome.
💡 Why this matters: The study helps connect several areas of cancer research, nutrition, the microbiome, microbial metabolism and immunotherapy. In the future, researchers may be able to develop carefully designed diets, bacterial therapies or microbial metabolites that help prepare the immune system to respond more effectively to treatment. @Nature @NatureMedicine @mcgillu @MIM_immuno @CRCHUM @chumontreal @UMontreal @uMontreal_news @med_umontreal @LysDesharnais @mcgillgci
Read more: https://t.co/vm9sGHYjyD


⚡ Science Saturday
Gas yield is a key indicator of digester performance. Stable biological conditions help maximize energy production while improving treatment efficiency.
#ScienceSaturday #Biogas #RenewableEnergy #Wastewater #AnaerobicDigestion
🧬 #ScienceSaturday
❓ What if cancer treatment decisions could be guided not only by the tumor cells themselves, but by the ecosystem around them?
➡️ A new study in @Nature introduces a machine-learning approach to study the tumor microenvironment, or the “neighborhood” around tumor cells made up of immune cells, blood vessel cells, fibroblasts and other supporting cells.
➡️ Researchers analyzed more than 10 million single-cell and spatial transcriptomic profiles across multiple cancer types to understand not only which cells are present in tumors, but where they are located and how they interact.
➡️ They identified nine recurring “spatial ecotypes,” or tumor neighborhoods, each with distinct biology and location patterns. Some were found near the tumor core, others at the tumor edge or surrounding tissue.
➡️ Importantly, some of these tumor neighborhoods were linked to patient outcomes and response to immune checkpoint inhibitors, a type of immunotherapy that helps the immune system recognize and attack cancer.
➡️ The most exciting part: the team showed that these spatial patterns could also be detected using cell-free DNA from blood samples, offering a potential non-invasive way to better understand the tumor microenvironment.
➡️ In patients with melanoma, these blood-based signals were strongly associated with response to immunotherapy, suggesting this approach could one day help guide treatment decisions.
💡 The takeaway: tumors are more than just cancer cells. Their surrounding ecosystem plays a major role in how cancer grows, hides and responds to treatment. This study points to a future where liquid biopsies may help us read that ecosystem in real time, bringing us closer to more personalized cancer care.
@AaronNewmanLab @Stanford @czbiohub @MayoClinic @Yale @rondell_graham @YaleGenetics @YaleCancer @SmilowCancer @StanfordCancer @Columbia @columbiacancer @columbiamed @MedicalCollege @Oslounivsykehus @WashUMedicine @UniOslo @WilmotCancer
Read more: https://t.co/OOwjAAFtzm

🌱 Science Saturday
Anaerobic digestion doesn't eliminate all solids. The material that remains is called digestate, and managing it effectively is an important part of overall system performance.
#ScienceSaturday #Biogas #Digestate #Wastewater #AnaerobicDigestion

@NASA's Cassini-Huygens mission to Saturn lasted from 1997-2015, and generated volumes of new data and hundreds of thousands of new images of the ringed planet and its nearly 300 satellites. Click through to learn more. #ScienceSaturday 🦟 ❤️ 🛰️
https://t.co/QA1ZAJAD6I

$NWBO #𝗗𝗖𝗩𝗮𝘅-𝗟: ��𝗵𝗲 𝗘𝘃𝗶𝗱𝗲𝗻𝗰𝗲 𝗶𝗻 𝗣𝗹𝗮𝗶𝗻 𝗧𝗲𝗿𝗺𝘀
A short, plain-language reading of the survival evidence for DCVax-L in #glioblastoma, and what it means under the @MHRAgovuk guideline on external control arms.
📊 𝗣𝗔𝗥𝗧 𝗢𝗡𝗘: 𝗪𝗛𝗔𝗧 𝗧𝗛𝗘 𝗧𝗥𝗜𝗔𝗟 𝗙𝗢𝗨𝗡𝗗, 𝗔𝗡𝗗 𝗪𝗛𝗬 𝗜𝗧 𝗠𝗔𝗧𝗧𝗘𝗥𝗦
DCVax-L more than doubled five-year survival, and the benefit is durability: a subset gets lasting disease control and simply stays alive.
💉 𝗪𝗵𝗮𝘁 𝘁𝗵𝗲 𝗱𝗿𝘂𝗴 𝗶𝘀
DCVax-L is a personalized cancer vaccine for glioblastoma, the deadliest form of brain cancer and a designated orphan disease. It is a living drug: its active ingredient is the patient's own immune cells, primed with proteins from that patient's surgically removed tumor, so the immune system learns to attack the cancer. Unlike a chemical drug that is metabolized and cleared, it switches on a living immune response that keeps working long after the injection. Glioblastoma comes back in almost everyone: even with the full standard of surgery, radiation, and temozolomide chemotherapy, most patients live under two years, and only about one in twenty reaches five. DCVax-L is given on top of that standard care, not in place of it: every patient in the trial received surgery, radiation, and temozolomide, and the vaccine was added to it, so the comparison measures what the vaccine adds. For two decades, nearly every new drug tried in this disease has failed. That is the backdrop against which any positive result must be judged.
📈 𝗪𝗵𝗮𝘁 𝘁𝗵𝗲 𝘁𝗿𝗶𝗮𝗹 𝗳𝗼𝘂𝗻𝗱
In a Phase 3 trial of 331 patients, those who received DCVax-L lived longer. At the median the gain looks modest, about three months (19.3 versus 16.5). The number that matters sits at the far end of the survival curve: more than twice as many vaccine patients were alive at five years, 13.0% versus 5.7%, and a few reached ten years in a disease that usually kills within three. In patients whose tumor had already returned, the effect was larger still, cutting the risk of death by about 42%.
👥 𝗘𝘃𝗲𝗿𝘆 𝗴𝗿𝗼𝘂𝗽 𝗯𝗲𝗻𝗲𝗳𝗶𝘁𝗲𝗱, 𝗲𝘃𝗲𝗻 𝘁𝗵𝗲 𝗵𝗮𝗿𝗱𝗲𝘀𝘁 𝘁𝗼 𝘁𝗿𝗲𝗮𝘁
The benefit was not confined to the easy cases. Of the six prespecified subgroups the trial examined, every single one favored DCVax-L, and there was no group in which it did worse than standard care. The largest gains came in patients whose tumors carry MGMT methylation, who reached a median survival of 30.2 months from randomization against 21.3 for the controls. But even the hardest-to-treat patients, whose tumors lack that methylation, resist standard chemotherapy, and carry the worst prognosis in this disease, still came out ahead with the vaccine, at a hazard ratio of 0.93. A treatment that helps across the whole population, and helps most where the biology is most favorable, is acting like a real drug.
📉 𝗪𝗵𝘆 𝘁𝗵𝗲 𝗺𝗲𝗱𝗶𝗮𝗻 𝗵𝗶𝗱𝗲𝘀 𝘁𝗵𝗲 𝗿𝗲𝗮𝗹 𝘀𝘁𝗼𝗿𝘆
That five-year number is the whole story, and the median buries it. Almost every treatment that ever helped in glioblastoma did the same modest thing: it slid the survival curve a few months to the right, then let it fall back. Doubling five-year survival is different in kind.
A three-month gain at the median cannot, by itself, double the fraction alive at five years. The only shape that produces both numbers is a split: most patients get the small delay the median measures, while a subset gets durable disease control that lasts for years, well past where glioblastoma should have ended them. That subset is the long tail of the curve, and it is where the benefit lives.
A median ignores extremes, the way a town's median income tells you nothing about its millionaires. The real story is not a longer delay; it is that a meaningful share of patients simply stay alive.
🧬 𝗪𝗵𝘆 𝘁𝗵𝗲 𝗯𝗶𝗼𝗹𝗼𝗴𝘆 𝗽𝗿𝗲𝗱𝗶𝗰𝘁𝘀 𝘁𝗵𝗶𝘀 𝘀𝗵𝗮𝗽𝗲
The tail is not luck. It is what this biology is built to produce. The vaccine carries proteins from the patient's own tumor, so it aims the immune system at whatever that tumor is made of, not a fixed short list of targets. And it amplifies: one trained immune cell drives many others that multiply into cancer-killers.
Andres Salazar, the neurologist who developed poly-ICLC into the clinical adjuvant given with the vaccine, puts it in a line: you start the fire, and you keep it burning. A response like that does not produce a one-time bump. It builds and widens over time.
What matters is not just that a response forms, but what kind. Dendritic cells are the immune system's master switch for that, the cells that set what kind of attack the body mounts, and this vaccine is built from them. It drives what immunologists call a type 1 polarized response: an interferon-driven, cytotoxic program aimed squarely at the tumor. That direction comes from the vaccine itself; the poly-ICLC adjuvant given with it drives the same interferon program and sustains it. That is the active ingredient, and it has been measured. In UCLA studies of this approach, the patients whose immune systems mounted the strongest interferon response lived the longest. The response also spreads. In a different cancer, a vaccine carried on this same poly-ICLC adjuvant drove more than 70% of a patient's cancer-killing T cells to target proteins that were never in the vaccine: the immune system outgrew its original targets and went after the rest of the tumor on its own. This is called epitope spreading, and it is not particular to one tumor; it is what this kind of response does, and it is the kind of response DCVax-L builds. That breadth is the likeliest thing separating the long-term survivors from everyone else, a response that breaks past its targets and clears the disease rather than one that stays caged and stops.
There is even a tell in who benefits most: the effect is largest in tumors whose biology builds up more mutations under chemotherapy, and more mutations mean more targets for a whole-tumor vaccine to find. The same logic explains what the vaccine is not, and what it does not need. Checkpoint inhibitors, the drugs that release the immune system's brakes, have failed on their own in glioblastoma because there was no active response to release; the vaccine supplies that response first.
That makes the vaccine the natural foundation for combination therapy. Combining it with its poly-ICLC adjuvant, made by Oncovir, has already shown meaningful survival gains in a published analysis. In the pivotal trial, the vaccine's proven benefit came added on top of standard chemotherapy and radiation; the newer question is how much the immune response can carry on its own. A UCLA trial is now testing that in patients whose tumors have returned, adding #Keytruda (pembrolizumab), the checkpoint antibody from $MRK, in a regimen built entirely around the immune response with no chemotherapy or radiation in it at all. Its interim survival curve shows the shape the biology predicts. In the arm given the vaccine and Keytruda together after surgery, the curve does not fall away but flattens into a plateau, with roughly 65% of patients still alive well past the point where recurrent glioblastoma kills nearly everyone. That plateau is the signature of a response that took hold and lasted, the type 1 attack forming durable immune memory so that once the disease is controlled it stays controlled. That is where this points, and where it is already arriving, a treatment that works through the response itself, one that could in time lean less on the harsh radiation and chemotherapy that have defined glioblastoma care and barely moved its survival. These are interim results, from Prins, Cloughesy, and Liau at UCLA.
🔍 𝗣𝗔𝗥𝗧 𝗧𝗪𝗢: 𝗜𝗦 𝗜𝗧 𝗥𝗘𝗔𝗟?
The trial was randomized, an independent experiment shows the outside comparison is trustworthy, and every separate check points the same way.
🤔 𝗧𝗵𝗲 𝗼𝗯𝗷𝗲𝗰𝘁𝗶𝗼𝗻, 𝗮𝗻𝗱 𝘄𝗵𝘆 𝗶𝘁 𝗺𝗶𝘀𝘀𝗲𝘀 𝘁𝗵𝗲 𝗺𝗮𝗿𝗸
So much for what happened; the harder question is whether to believe it. The trial has the feature critics attacked: it could not keep a normal placebo group, because patients assigned to placebo were allowed, by design and by medical ethics, to switch to the vaccine once their cancer returned, and almost all did. That erased the internal comparison, so survival was measured against closely matched patients from other completed trials, an approach called an external control, which critics argued could tilt toward the vaccine.
What the objection misses is where the randomization went. This was a randomized, blinded trial. The patients who got the vaccine were assigned to it at random, not hand-picked, so the treated group is an ordinary slice of the trial population, not a favorable one. The crossover removed the placebo group but never touched how patients were assigned. That leaves exactly one place for bias to enter, the outside comparison group, which is precisely what the next checks test.
✅ 𝗧𝗵𝗲 𝗰𝗵𝗲𝗰𝗸 𝘁𝗵𝗮𝘁 𝗺𝗮𝗸𝗲𝘀 𝗶𝘁 𝘁𝗿𝘂𝘀𝘁𝘄𝗼𝗿𝘁𝗵𝘆
Before trusting a scale to weigh something unknown, you confirm it reads zero with nothing on it. That is what the calibration does, and it is the strongest part of the case. A separate, independent randomized trial called INSIGhT was run through the very same external-control method, and it gave two answers.
First, three experimental drugs that had already failed were run through it, and it correctly found nothing (hazard ratios of 1.00, 0.93, and 0.88): the method does not manufacture a benefit where none exists. Second, INSIGhT's external controls were set head to head against its own randomized internal controls, and they were statistically indistinguishable. In this disease, an external control reproduces the answer a real randomized control would have given, and because that trial belonged to a different group, no one can say a sponsor graded its own work. The one place bias could enter, the control side, is the one place an independent randomized experiment certified as clean.
There is a deeper fit worth naming, and it is what makes the two halves of this case one. The same instrument that reported those three failures as failures reads the vaccine as a success, and the biology says why: those drugs could not hold a tumor this varied, and the vaccine builds the broad, lasting response that finally does. One method, opposite readings, and one mechanism behind both. The statistics and the biology are not two arguments. They are the same argument seen twice.
🃏 𝗪𝗮𝘀 𝘁𝗵𝗲 𝗰𝗼𝗺𝗽𝗮𝗿𝗶𝘀𝗼𝗻 𝘀𝘁𝗮𝗰𝗸𝗲𝗱 𝗶𝗻 𝘁𝗵𝗲 𝘃𝗮𝗰𝗰𝗶𝗻𝗲'𝘀 𝗳𝗮𝘃𝗼𝗿?
A natural worry is that the outside comparison was arranged after the fact to flatter the vaccine. The trial was built to prevent that. The patients to compare against, and the rules for matching them, were fixed in writing before anyone saw results, and an independent firm, not the company, chose the comparison trials against those rules. The trial also switched its main measure partway through, from delaying tumor growth to overall survival, but that was not a maneuver: immune treatments cause a harmless swelling that mimics tumor growth on scans and made the growth measure unreliable, and the switch was made while everyone was still blinded.
Three further checks point the same way. Survival in this disease has not improved over the years the comparison spans, so same-era controls are sound. When the borrowed controls were tested directly, the comparison came out conservative rather than flattering. And the controls were counted from the same point in the disease as the vaccine patients, so neither side got a head start. Where the comparison can err, it errs against the drug.
🔬 𝗧𝗵𝗲 𝗺𝗼𝗿𝗲 𝗰𝗮𝗿𝗲𝗳𝘂𝗹 𝗮𝗻𝗮𝗹𝘆𝘀𝗶𝘀 𝗺𝗮𝗱𝗲 𝘁𝗵𝗲 𝗯𝗲𝗻𝗲𝗳𝗶𝘁 𝗯𝗶𝗴𝗴𝗲𝗿, 𝗻𝗼𝘁 𝘀𝗺𝗮𝗹𝗹𝗲𝗿
The first comparison used whole groups. A sharper one became possible once patient-level records from three other trials could be obtained, pairing each vaccine patient with controls matched on the traits that drive survival in glioblastoma, above all MGMT methylation status, matched exactly, plus age, sex, extent of surgery, residual disease, and performance status. When the comparison got sharper, the benefit grew in every one of these analyses. The original cohort-level estimate was 2.8 months. Patient-level matching across the three trials put the gain between 3.4 and 6.3 months, and a method that weights patients rather than pairing them put it between 3.4 and 4.3, with several of the matched comparisons roughly doubling the original figure. The hazard ratio moved the same way, from 0.80 to between 0.69 and 0.77.
The direction matters. A real effect blurred by crude matching gets clearer when the matching improves, while a biased one tends to shrink. It got stronger.
🕵️ 𝗛𝗼𝘄 𝗺𝘂𝗰𝗵 𝗵𝗶𝗱𝗱𝗲𝗻 𝗯𝗶𝗮𝘀 𝘄𝗼𝘂𝗹𝗱 𝗶𝘁 𝘁𝗮𝗸𝗲 𝘁𝗼 𝗲𝘅𝗽𝗹𝗮𝗶𝗻 𝘁𝗵𝗶𝘀 𝗮𝘄𝗮𝘆
A fair question is how much hidden bias it would take to erase the result. Statisticians measure that with the E-value, and here a hidden factor would have to be about as strong as age is on survival, would also have to drive who received the vaccine, and would have to have escaped the decades of research that mapped every known risk factor in this disease. A second, independent check, Rosenbaum's Gamma, comes at it from the other side, asking how large an unseen imbalance between matched patients it would take to break the result, and it reaches the same verdict. Every factor strong enough to matter was already matched. A hidden one that clears that bar is not plausible.
🔒 𝗪𝗵𝘆 𝘁𝗵𝗲 𝗿𝗲𝘀𝘂𝗹𝘁 𝗶𝘀 𝗵𝗮𝗿𝗱 𝘁𝗼 𝗳𝗮𝗸𝗲
The strongest point is not any single result. It is that a hidden bias big enough to explain the effect away would have to produce the same answer in every independent test at once:
• The independent randomized calibration trial.
• Three separate comparison trials, drawn from different studies.
• Two different statistical methods that handle the data in different ways.
• A separate pooled analysis of other dendritic-cell vaccine trials.
• The internal math of the survival curve, which points to the same result (about 0.71 at five years) that the patient matching found.
And it would have to fall in the exact direction the biology predicted before any data existed: a slow, widening benefit concentrated in long-term survivors. A single hidden factor that could forge all of that at once is not a hidden factor. It is a coincidence that does not happen.
🩺 𝗣𝗔𝗥𝗧 𝗧𝗛𝗥𝗘𝗘: 𝗪𝗛𝗔𝗧 𝗜𝗧 𝗠𝗘𝗔𝗡𝗦
The drug is nearly free of harm, the evidence fits an established and approved regulatory path, and what remains unrun changes nothing about the case.
🛡️ 𝗧𝗵𝗲 𝘀𝗮𝗳𝗲𝘁𝘆
Two things decide whether a real effect reaches patients: whether the drug is safe enough to use, and whether regulators will accept the evidence. The first is settled. Across 2,151 doses, only five serious side effects were even possibly related to the vaccine, with no autoimmunity and no cytokine storm. It is made once, in about eight days, then stored and given as a simple injection. When a treatment barely harms, the benefit needed to justify it falls, and the benefit here clears that lower bar easily.
⏳ 𝗪𝗵𝘆 𝘁𝗵𝗲 𝘀𝘁𝗿𝗼𝗻𝗴𝗲𝗿 𝗱𝗮𝘁𝗮 𝗮𝗽𝗽𝗲𝗮𝗿𝗲𝗱 𝗼𝗻𝗹𝘆 𝗻𝗼𝘄
A reasonable person asks why the sharper analysis appeared in 2026 and not in 2023. The answer is access, not choice. The patient-level analysis was written into the trial's plan from the start, to run if and when the data could be obtained. The company tried and could not get it in 2023, because the trials that held it had not released it; it became available later through a data-sharing repository, on the data owners' timeline, not the company's. The stronger analysis was always the plan. It was waiting on data that other parties control.
🔄 𝗣𝗮𝘁𝗶𝗲𝗻𝘁𝘀 𝘄𝗵𝗼𝘀𝗲 𝗰𝗮𝗻𝗰𝗲𝗿 𝗿𝗲𝘁𝘂𝗿𝗻𝗲𝗱 𝗮𝗹𝘀𝗼 𝗯𝗲𝗻𝗲𝗳𝗶𝘁𝗲𝗱
The vaccine helped not only newly diagnosed patients but also those whose tumor had already come back, and there the effect was the largest seen anywhere in the trial. In that group, median survival ran 13.2 months from recurrence against 7.8 for the controls. The separation opened immediately, with 90.6% of vaccine patients alive at six months against 64.0% of controls, and the lead held to the later marks, where survival more than doubled: 20.7% against 9.6% at two years, 11.1% against 5.1% at two and a half. These are the original cohort-level results, already published. The high-resolution patient-level matching that was applied to the newly diagnosed group has not yet been done here, for a practical reason: it needs patient records from other recurrent-cancer trials, held by a European research organization that shares them through its own formal request. Obtaining them is a routine next step, not an obstacle, and the newly diagnosed experience suggests the sharper analysis would only make the recurrent result stronger. The approval case rests on the newly diagnosed evidence, so nothing important depends on this step; it would simply sharpen a result that is already the strongest in the trial.
🏛️ 𝗪𝗵𝗮𝘁 𝘁𝗵𝗶𝘀 𝗺𝗲𝗮𝗻𝘀 𝗳𝗼𝗿 𝗮𝗽𝗽𝗿𝗼𝘃𝗮𝗹
Regulators do not treat an external control as a first choice, but the MHRA's guideline allows it in exactly this situation: a severe disease where a placebo trial is not ethical or feasible, and an effect large enough to interpret despite the design. The guideline even gives its own worked example of an acceptable external control, and it reads almost like a description of this trial: a rare disease, no ethical placebo, same-era standard-of-care controls, an objective survival endpoint, and an effect too large to blame on bias. DCVax-L fits on every count, and it was the first medicine ever to receive the MHRA's Promising Innovative Medicine designation, which asks essentially the same questions. The newly diagnosed case carries the decision on its own evidence, and regulators weigh that evidence against the disease it treats: in a cancer this lethal, with nothing better on offer, the question is whether the benefit is large, clear, and consistent enough to act on, and a benefit of this size, pointing the same way from every direction, is.
📜 𝗧𝗵𝗶𝘀 𝗵𝗮𝘀 𝗯𝗲𝗲𝗻 𝗱𝗼𝗻𝗲 𝗯𝗲𝗳𝗼𝗿𝗲, 𝗮𝗻𝗱 𝗮𝗽𝗽𝗿𝗼𝘃𝗲𝗱
External controls are not a novelty invented for this drug. Over the past two decades they have factored into roughly forty-five drug approvals by the United States regulator, each granted under the conditions that apply here: a serious or rare disease, a placebo that would be unethical, and high unmet need. Regulators do not grant this lightly. They grant it when the disease is serious, its course is predictable and objectively measured, and the effect is large. Glioblastoma meets all three.
The named cases cover every part of this disease's profile. Defibrotide, for a life-threatening transplant complication, was approved on a propensity-score comparison to a historical control, the same kind of method used here. Blinatumomab, for an aggressive relapsed leukemia, is the precedent for a fast-killing cancer, cleared by both the United States and European regulators. Cerliponase alfa is the precedent for a fatal brain disease, cleared by both agencies on treated patients versus a matched natural-history group. Glioblastoma is both at once, a fast-killing cancer of the brain, read by the same method, so no part of its profile lacks a close approved precedent.
And on the one axis that governs how far an external-control result can be trusted, DCVax-L goes beyond all three. Each of those drugs was tested in a single-arm trial, with no randomization at all. DCVax-L began as a randomized trial and became an external-control comparison only when ethics consumed its placebo group. It sits in that tradition, and at the top of it.
🎯 𝗧𝗵𝗲 𝗯𝗼𝘁𝘁𝗼𝗺 𝗹𝗶𝗻𝗲
This began as a randomized trial. Medical ethics forced it into an external-control comparison. Every independent way of checking it, on different data and different math, points the same direction, and the biology predicted that direction in advance. The first analysis did not overstate the vaccine's effect. Read with the right tools, it understated it.

🧬 #ScienceSaturday
❓ What if treating brain cancer means targeting not just the tumor, but the cells helping it hide?
➡️ A new study in @Nature explores a promising CAR T-cell strategy for glioblastoma, one of the most aggressive and difficult-to-treat brain cancers.
➡️ Glioblastoma is especially challenging because it is not made up of identical cancer cells. It is a complex ecosystem, with tumor cells that can vary from one another and immune cells in the surrounding environment that can be “reprogrammed” to support the cancer instead of fighting it.
➡️ Researchers focused on a target called GPNMB, which they found on both glioblastoma tumor cells and tumor-associated macrophages, immune cells that can help create an immunosuppressive environment around the tumor.
➡️ They then engineered #CART cells to recognize GPNMB. In preclinical models, these CAR T cells were able to attack both the cancer cells and the tumor-supporting macrophages.
➡️ This dual approach is important because many CAR T-cell strategies for glioblastoma have struggled when tumors lose the target or use the surrounding immune environment to resist treatment.
➡️ By targeting both the #tumor and part of its protective neighborhood, this strategy may offer a new way to think about treating glioblastoma and other solid tumors with complex, immune-suppressive environments.
➡️ The study is still early and was tested in preclinical models, not patients. But it points to an exciting idea: future therapies may need to treat cancer not just as a mass of tumor cells, but as an ecosystem that must be disrupted from multiple angles.
The future of #cancer treatment may depend on understanding not only the cancer itself, but also the cells helping it survive. @sheilasinghlab @McMasterU @McMasteResearch @machealthsci @UCalgaryMed @NorthwesternMed @HamHealthSci @UofT @LurieCancer @Charb_Cancer
Read more here: https://t.co/p0uyU58LPm

🧬 #ScienceSaturday
❓ Why are more cancers being diagnosed in younger adults?
➡️ A new study in @NatureMedicine suggests one possible clue may be biological aging, how “old” the body appears based on blood, metabolic and protein markers, not just birthdays.
➡️ Researchers analyzed more than 154,000 young adults in the UK Biobank and also validated part of their findings using the U.S. All of Us Research Program.
➡️ They found that people born in more recent generations showed signs of greater biological #aging compared with earlier birth cohorts.
➡️ They also found that a higher biological “age gap”, meaning the body appears older than expected for someone’s actual age, was associated with a higher risk of early-onset solid cancers.
➡️ This was especially seen in lung, gastrointestinal/colorectal and uterine cancers.
➡️ The study also looked at organ-specific aging. Immune system aging was linked to early-onset lung #cancer, while adipose tissue aging was linked to early-onset colorectal cancer.
🧠 Why this matters: Early-onset cancers are rising, but the reasons are still not fully understood. This study does not prove that accelerated biological aging causes cancer, but it suggests it may be an important signal of the cumulative effects of lifestyle, environment, #inflammation, #metabolism and other exposures.
✨ Big takeaway: Cancer risk is not only about how many years we have lived. It may also be shaped by how our bodies age over time, and understanding that process could help researchers find new ways to prevent and detect cancers earlier.
Read more here: https://t.co/Q1zcfyNX6x
@Nature @washumedicine @SitemanCenter @WashU @WUSTLphs @JD_Buenrostro @harvardmed @Harvard @broadinstitute @Seye_Oduyale @DanielYHongMD @STicaMDMPH @RuiyiT

🧬 #ScienceSaturday
❓ What if a #virus could be trained to recognize #cancer cells and only attack when it detects their abnormal growth signals?
➡️ In a new study published in Nature #Biomedical #Engineering, researchers engineered a “smart” virus designed to activate only in cancer cells with overactive ErbB/HER2 signaling, a growth signal that is abnormally switched on in some ovarian, breast, pancreatic, and other cancers.
➡️ The team built an engineered virus called ErbB-OSV. Instead of copying itself everywhere, this virus was rewired so it can replicate mainly inside cancer cells with this abnormal growth signal. Once activated, the virus multiplies inside the cancer cell and helps destroy it.
➡️ In mouse models of metastatic ovarian cancer, ErbB-OSV was more selective and safer than a standard cancer-killing virus. It also worked especially well when combined with standard chemotherapy, helping control tumors and extend survival more than chemotherapy alone.
➡️ Most strikingly, when treatment was started earlier in one mouse model, ErbB-OSV appeared to eliminate the tumors in all treated mice.
💡 Why this matters:
Many cancer treatments can harm healthy cells because they target features that normal cells may also have. This approach is exciting because it targets a cancer cell’s abnormal behavior, its overactive growth signaling, and uses that signal as the “on switch” for treatment.
This study points to a powerful idea: future cancer therapies may be engineered to sense cancer’s internal wiring and attack only when the right danger signal is present. @NatureCancer @Nature @natBME @Stanford @StanfordMed @michaelzlin @MichaelLinLab @WesternU @StanfordCancer @StanfordHealth
Read more here: https://t.co/O10OEdh47I

🧬 #ScienceSaturday
❓ Why does immunotherapy work so well for some cancers, but often fail in #glioblastoma, one of the most aggressive brain cancers?
➡️ A new study in @NatureCancer suggests the answer may depend less on how many DNA mutations a tumor has, and more on the tumor’s “cell state,” or what the cancer cells are actively doing.
➡️ Researchers studied 181 glioblastoma samples from patients treated with immune checkpoint blockade, a type of immunotherapy designed to help T cells recognize and attack cancer.
➡️ They found that glioblastomas in a mesenchymal, or MES, state were linked to better survival after immunotherapy. These tumors appeared more “immune-visible,” with higher levels of HLA class I, a signal that helps T cells recognize abnormal cells, and more T cell infiltration.
➡️ Surprisingly, #tumor mutational burden, a marker often used to predict immunotherapy response in other cancers, did not predict better outcomes in this glioblastoma group.
➡️ The study also revealed a possible escape route: after #immunotherapy, some tumors shifted away from the MES state toward non-MES states, which may make them less recognizable to the immune system and more resistant to treatment.
🧠 Why this matters: Glioblastoma has been extremely difficult to treat, and checkpoint immunotherapy has mostly been disappointing in this disease. This study suggests that future trials may need to look at a tumor’s RNA “activity pattern,” not just its #DNA mutations, to identify patients who may be more likely to benefit.
✨ Big takeaway: In glioblastoma, the tumor’s current “state of mind” may help predict whether immunotherapy can see it, attack it, and make a difference.
Read more here: https://t.co/o2Y1JVSdGy
@Nature @DanaFarber @Harvard @harvardmed @MassGenBrigham @broadinstitute @IBMResearch @DanaFarberNews @EAChiocca @JackYGhannam

🧬 #ScienceSaturday
❓ What if a simple blood test could reveal that the lungs are becoming “cancer-friendly” years before #lung cancer is diagnosed?
➡️ In a new study published in @CellCellPress, researchers found a 14-protein signal in blood plasma that helped predict future lung cancer risk, sometimes more than 5 years before diagnosis.
➡️ These proteins were not just signs of an existing tumor. Instead, they seemed to reflect an inflamed lung environment, one that may help early cancer-prone cells survive and grow.
➡️ The team found that air #pollution, smoking-related inflammation, EGFR cancer-driving mutations, and a molecule called IL-1β could all raise parts of this protein signal.
➡️ They also studied a prevention trial involving canakinumab, a drug that blocks IL-1β. People with a high protein signature appeared more likely to benefit from this anti-inflammatory approach than people with a low signature.
🌟 This study suggests a future where cancer prevention could become more personalized: instead of treating everyone the same, doctors might use blood signals to identify who is most likely to benefit from prevention before #cancer fully develops.
🔗 Read the study: https://t.co/EvaXZWws9Y
@CharlesSwanton @DrClareWeeden @TheMarkFdn @TheCrick @ucl @SwantonLab @uclcancer

🧬 #ScienceSaturday
❓ Why do some colorectal cancers resist #immunotherapy, even when they should respond?
➡️ A new study in @CellCellPress explored how immune cells inside tumors interact and discovered that resistance to PD-1 blockade may be driven by suppressive macrophages and exhausted T cells.
➡️ Researchers found that successful responses were linked to coordinated activity between cancer-fighting T cells and immune-supporting macrophages that help activate anti-tumor immunity.
➡️ Tumors that resisted treatment showed higher levels of TREM2+ macrophages and multiple immune checkpoints, including LAG3 and CTLA4, creating an immunosuppressive tumor environment.
➡️ By combining PD-1 blockade with therapies targeting LAG3, CTLA4 and TREM2, researchers achieved complete tumor clearance in up to 100% of mismatch repair-deficient colorectal cancer models.
🌟 The findings highlight how reprogramming immune cell communication inside tumors could help overcome immunotherapy resistance and improve outcomes for more patients with colorectal cancer.
🔗 Read the study: https://t.co/V04qwJZSeq
@BhardwajLab @CimenBozkus_C @matt_brown04 @NatalieVaninov @SpitzerLab @neoviral @rsamstein @IcahnMountSinai @SinaiImmunol @MountSinaiNYC

🧬 #ScienceSaturday
❓ What if we could program cancer-fighting immune cells directly inside the body instead of making them in a lab?
➡️ A new study in @NatureComms shows a way to generate CAR T cells in vivo using engineered lentiviral vectors that deliver genetic instructions directly to T cells after being injected into the bloodstream.
➡️ To improve precision, the researchers redesigned the viral surface proteins so they more selectively bind to T cells. They also used camelid-derived nanobodies (VHHs), which act like highly specific molecular “guides,” to help the virus target the right cells.
➡️ They further modified the viral coat using a dolphin morbillivirus–based chimera to help it evade preexisting immunity to measles, which can otherwise block viral delivery in some people.
➡️ In preclinical models, a single systemic dose led to the body producing its own CAR T cells, which expanded and showed strong anti-tumor effects, including durable tumor control.
🌟 This approach moves CAR T therapy closer to an “in-the-body” manufacturing model, potentially removing the need for complex cell collection and lab-based engineering.
🔗 Read the study: https://t.co/6jprsxZ2Hf
@MangusoLab @KeplerMears @broadinstitute @MIT @MassGenBrigham
🧬 #ScienceSaturday
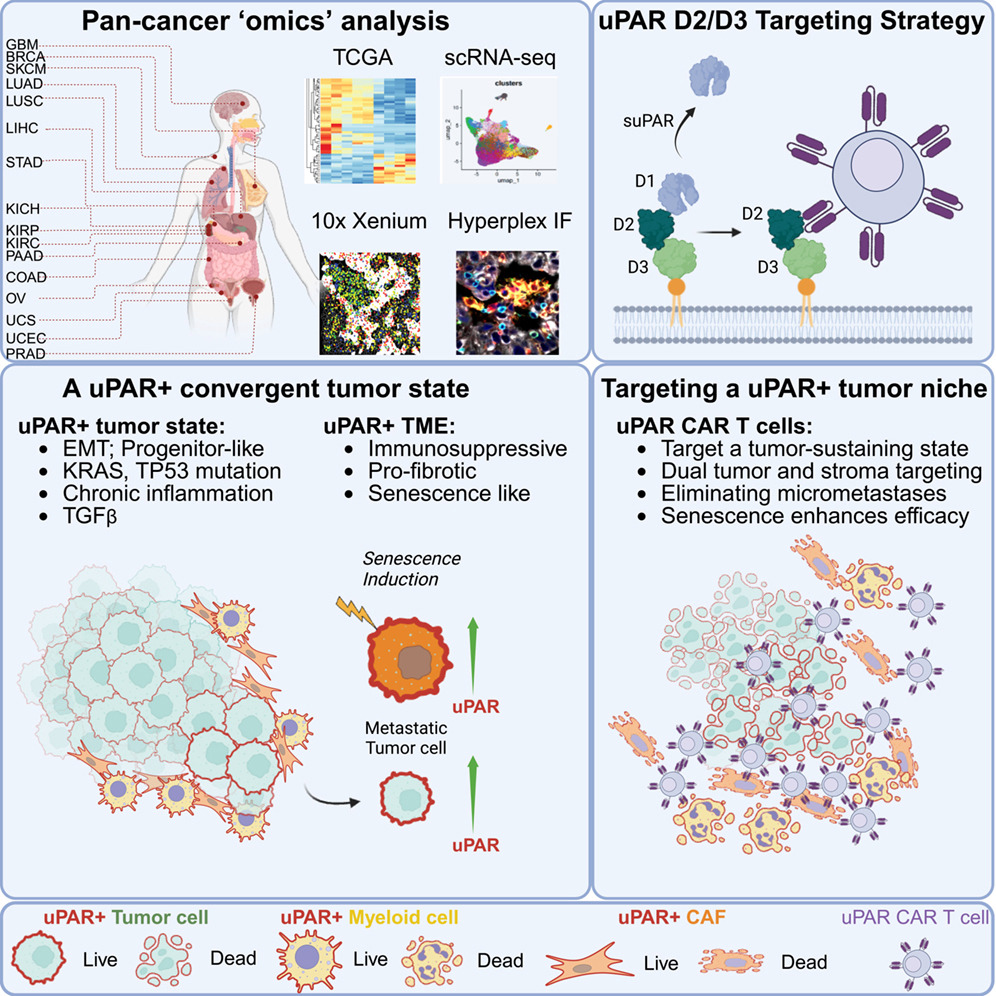
❓ What if cancer treatment could target not only tumor cells, but also the tumor’s stromal support: non-malignant, non-cancerous cells within the tumor microenvironment, that actively help cancer grow, spread, and resist treatment?
➡️ In a new study published in @CellCellPress, researchers identified uPAR, a cell-surface protein linked to aggressive tumor behavior, as a marker found on both solid tumor cells and the fibrotic, immune-suppressive environment that helps sustain them.
➡️ The team developed uPAR-targeted CAR T cells that attacked both tumor cells and their supportive stroma, leading to durable tumor regression across multiple cancer models, including metastatic disease.
➡️ They also found that senescence-inducing therapies, like chemotherapy, increased uPAR expression and made tumors even more vulnerable to CAR T cell treatment.
🌟 This dual-targeting strategy could help overcome some of the biggest barriers to CAR T therapy in solid tumors, including immune suppression and treatment resistance.
🔗 Read the study: https://t.co/dvHrEzUZ7F
@ZedaZhang @Aveline_Filliol @LoweLabMSKCC
#ScienceSaturday
❓ Why is it so rare for cancer to spread to the heart, and what can this teach us about suppressing tumors elsewhere in the body?
➡️ A new study in @ScienceMagazine shows the heart’s beating, a constant mechanical force, may actually suppress tumor growth. Cancer cells that reach the heart are exposed to intense physical stress, which alters gene expression and limits proliferation.
➡️ When researchers “unloaded” the heart in experimental models, tumors, including melanoma, grew more aggressively. Under normal conditions, mechanical stress activates mechanosensing pathways like Nesprin-2, which helps shut down cancer cell growth.
➡️ In melanoma, where metastases can reach almost anywhere in the body, cardiac involvement does occur, but is still rare. Have you encountered heart metastases in your practice?
🌟 This work helps explain why cardiac metastases are uncommon and points to an intriguing future, leveraging mechanical forces as a novel strategy to slow or stop cancer growth.
🔗 Read the full study in Science: https://t.co/q6v9EkTKv6
@SerenaZacchigna @CiucciGiulio @ICGEB


@sunset_coral SECME club took 3rd 🥉place #thrillit #quakeit @CoxSci #engineerit Great Job Ms. Mooney! @PBCSDSTEM @GarvinShaw @missy_reid2 @InstSupSteiger #STEM #sciencesaturday #proudtobeadolphin #girlsinstem



@sunset_coral SECME club took 1st place 🥇 in #dropit #cleanit #launchit @CoxSci #engineerit Great Job Ms. Mooney! @PBCSDSTEM @GarvinShaw @missy_reid2 @InstSupSteiger #STEM #sciencesaturday #proudtobeadolphin



🧬 #ScienceSaturday
❓ What if we could block cancer’s ability to survive in low-oxygen environments and make #immunotherapy more effective?
➡️ In a new study published in the Journal of Experimental Medicine (@JExpMed), researchers developed dual inhibitors targeting HIF-1 and HIF-2, key regulators that help tumors adapt to hypoxia.
➡️ These compounds bind HIF proteins, block their activity and trigger their degradation, shutting down pathways that drive tumor growth, angiogenesis and immune evasion.
➡️ In preclinical models, dual HIF inhibition suppressed tumor growth across multiple cancer types and outperformed selective HIF-2 inhibitors.
➡️ When combined with immune checkpoint blockade in murine models, response rates exceeded 50% and helped overcome resistance to immunotherapy.
🌟 Targeting #hypoxia may help reprogram the tumor microenvironment and unlock stronger immune responses.
🔗 Read the study: https://t.co/JqceQpWjlL
@JohnsHopkins @HopkinsMedicine @umsop @eewicks @onlyoscarli

🧬 #ScienceSaturday
❓ What if the “energy state” of an immune cell determines how well it can fight cancer?
➡️ In a new study published in @ScienceMagazine, researchers found that dendritic cells inside tumors exist in two mitochondrial states, and only the “high-energy” cells effectively activate CD8+ T cells.
➡️ These high-functioning cells rely on the OPA1–NRF1 pathway to sustain mitochondrial metabolism and preserve antigen presentation.
➡️ When this pathway breaks down, antigen presentation drops and anti-tumor immune responses weaken.
🌟 Reprogramming immune cell metabolism could help strengthen immunotherapy responses and overcome treatment resistance.
🔗 Read the study: https://t.co/kiHMMoFmRt
@hongbo_chi @StJude

Last Seen Hashtags on Sotwe
earthdancenairobi
Seen from United States
monkeyapp
Seen from Brazil
agegap
Seen from Saudi Arabia
nsfwtwtً
Seen from Jordan
แม่หม้าย
Seen from Thailand
bop
Seen from United States
omegle
Seen from Argentina
kıbrıspasif
Seen from Turkey
leaks
Seen from France
momson((())) filter:videos
Seen from Colombia
Most Popular Users

Elon Musk 
@elonmusk
240.9M followers

Barack Obama
@barackobama
119.2M followers

Donald J. Trump
@realdonaldtrump
111.8M followers

Cristiano Ronaldo
@cristiano
111.7M followers

Narendra Modi
@narendramodi
107.1M followers

Rihanna
@rihanna
97.9M followers

NASA
@nasa
92.2M followers

Justin Bieber
@justinbieber
91.1M followers

KATY PERRY
@katyperry
88.2M followers

Taylor Swift
@taylorswift13
82.1M followers

Lady Gaga
@ladygaga
73.6M followers

Virat Kohli
@imvkohli
70.8M followers

Kim Kardashian
@kimkardashian
70.1M followers

YouTube
@youtube
68.7M followers

Bill Gates
@billgates
64.2M followers

Neymar Jr
@neymarjr
63.7M followers

The Ellen Show
@theellenshow
62.4M followers

CNN
@cnn
61.8M followers

Selena Gomez
@selenagomez
61.3M followers

X
@x
60.8M followers