This paper by @drtanws @heerlab @emmahall71 provides supporting evidence removing TaHG NMIBC from the IR NMIBC risk category
When we properly define IR-NMIBC the way @IBCG_BladderCA recommends - LG disease only - and look at what happens to those patients across four RCTs (578 patients, contemporary treatment):
Stage progression: 2%
MIBC or metastasis: 2%
Cancer-specific mortality: <1%
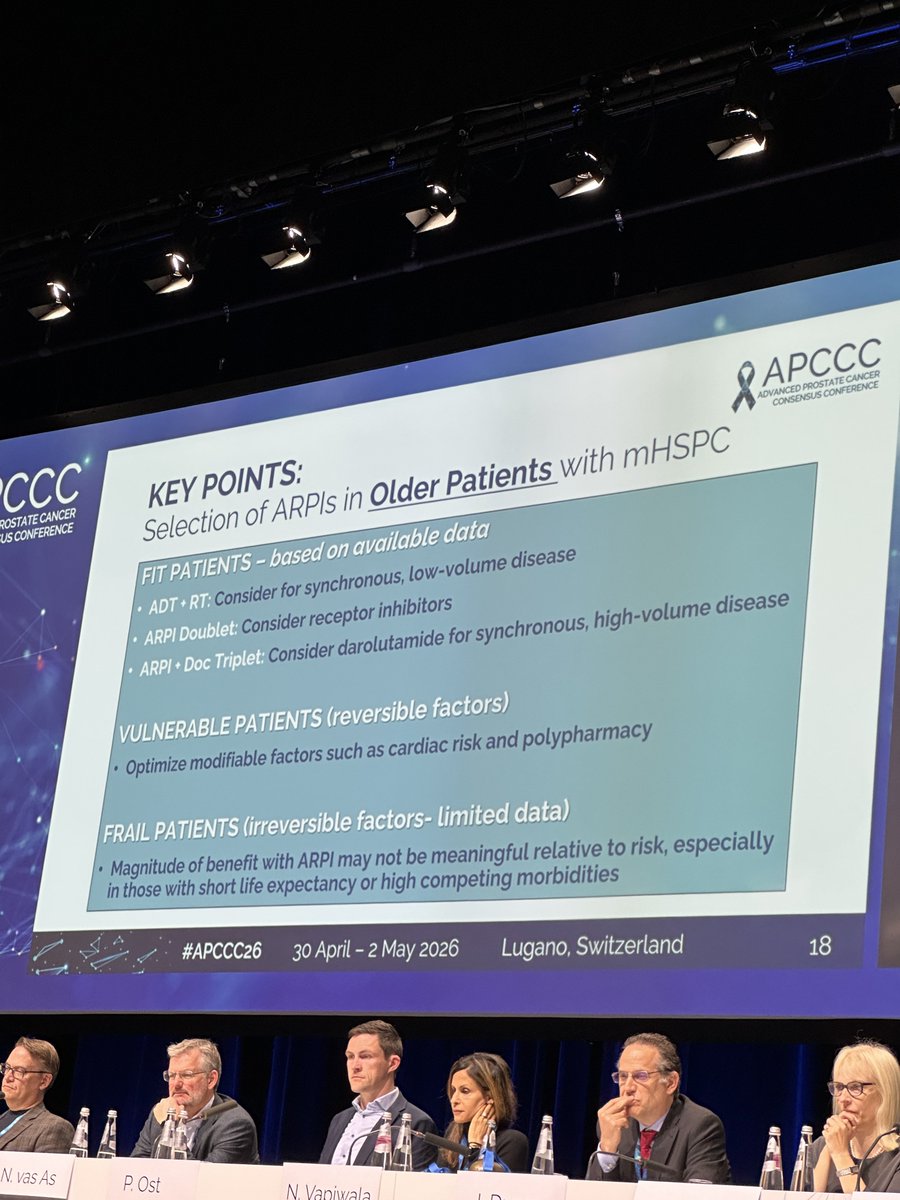
Can treatment be safely stopped in selected patients with mHSPC?
Phase II A-DREAM trial, 41% of responders remained treatment-free with testosterone recovery 18m after stopping ADT/ARPI. At a median FU of 21 months, 35% of patients required treatment re-initiation.
@OncoAlert
Can baseline testosterone levels help predict which prostate cancer patients on active surveillance are at higher risk of progression?
In this article, researchers found that low testosterone (≤300 ng/dL) was linked to increased risk of higher-grade progression (GG3 or above), suggesting it may be a valuable prognostic marker to guide surveillance and treatment decisions.
🔗 Click to read more: https://t.co/CwjENsPNc6
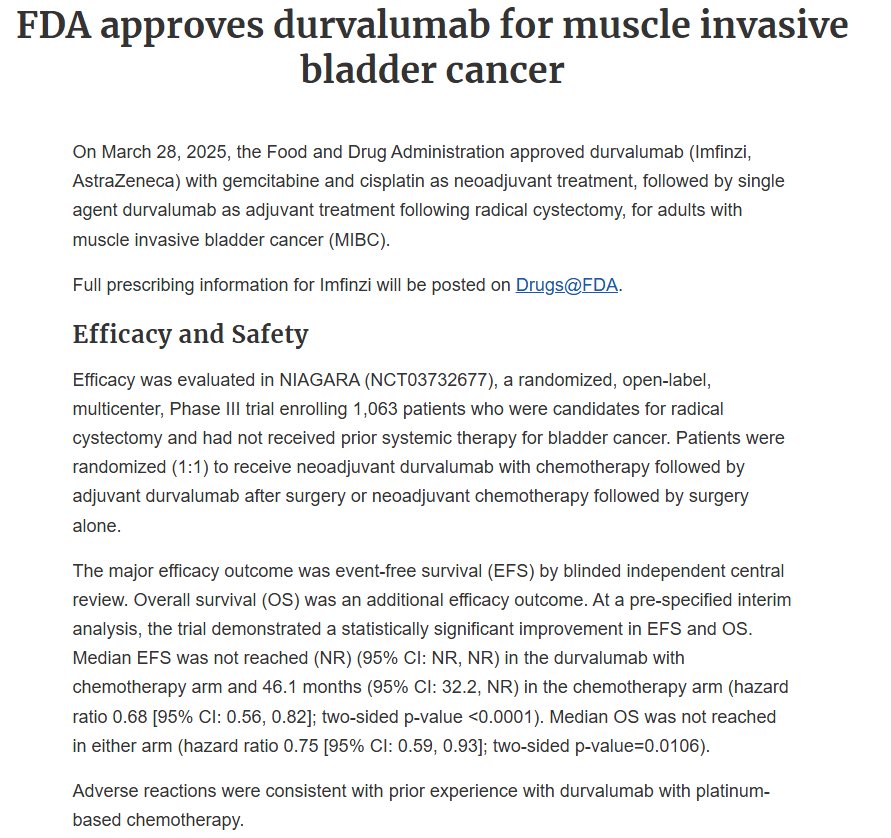
⚖️ Now put that 5% on a scale.
To move 5 more patients per 100 into the disease-free column at 2 years, you add 13 monthly IV infusions and a Grade 3/4 toxicity rate that jumps from 4% to 21%.
No OS benefit yet. Median DFS not reached in either arm.
How do we balance and offer personalized recommendations?
HR doesn’t make that decision for you. @WorldBladderCan@IBCG_BladderCA
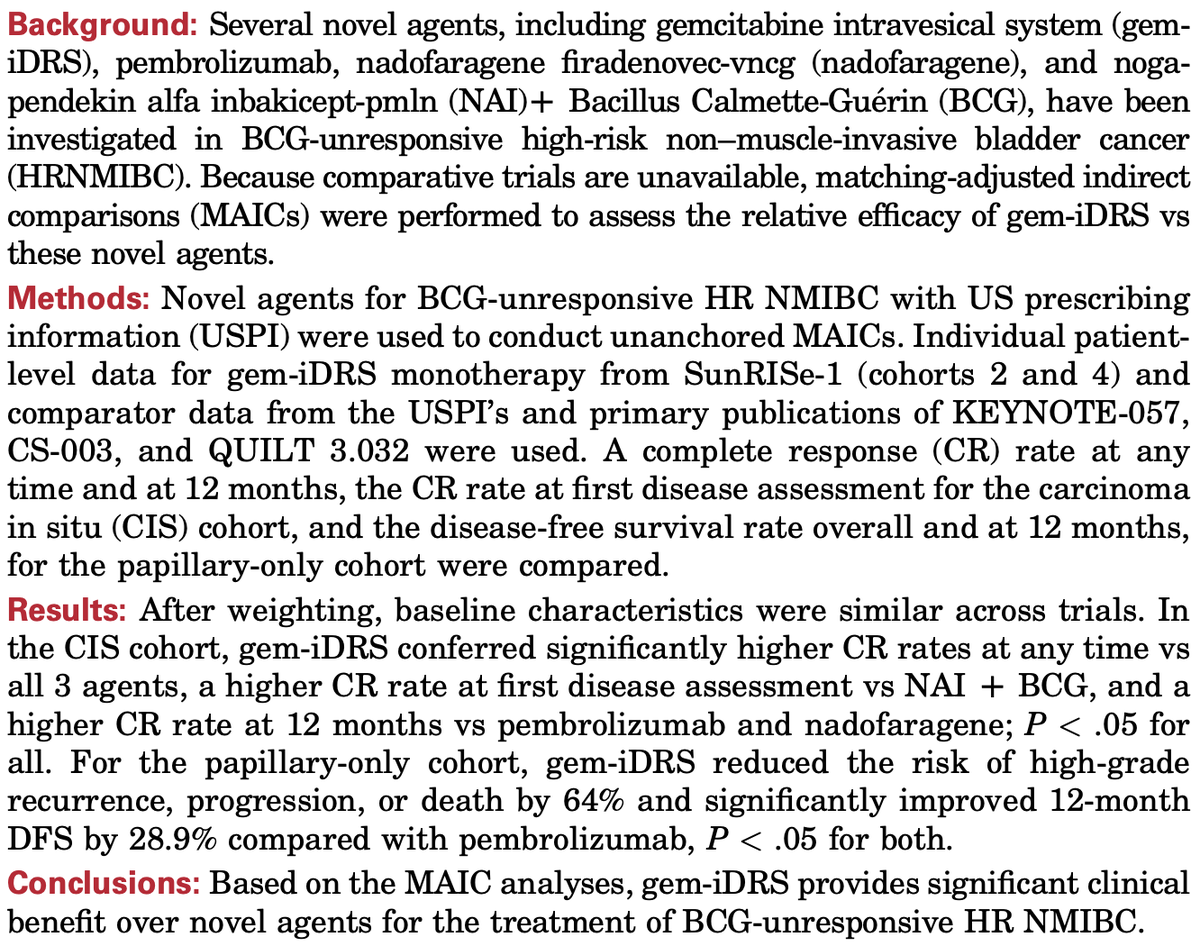
🚨A lot of new options for #BCGunresponsive NMIBC, but no direct comparisons
🤼We've tried to do some work on this, along with my friend @siadaneshmand and others
📖You can read it here @JUrology@AmerUrological@JUOpenPlus: https://t.co/Um9tDRn1UC
👀And much more to come!!!
En bloc cystectomy is proving to be a powerful approach in challenging cx> post-EV/P, bulky fibrotic disease and EV/P progressors ⬆️ R0 %, ⬇️ EBL and improved node # We keep expanding our robotic en bloc cystectomy experience with LN ctDNA measurement .. innovation in tx requires 🤖 innovation in approach . credit to @EirikKjo@CleClinicUro
#AUA26 First indirect comparison of two FDA-approved bladder-sparing strategies for BCG-unresponsive NMIBC: NAI + BCG vs TAR-200.
After MAIC adjustment:
🎯 12-mo CR:
• NAI+BCG: 49.2%
• TAR-200: 45.9%
⚠️ TRAEs:
• 61.7% with NAI+BCG
• 83.5% with TAR-200
→ ~68% lower odds of treatment-related toxicity with NAI+BCG (OR 0.32)
🚨No head-to-head trial yet, but an important attempt to compare emerging bladder-preserving options in BCG-unresponsive NMIBC. @UroToday @AmericanUrological
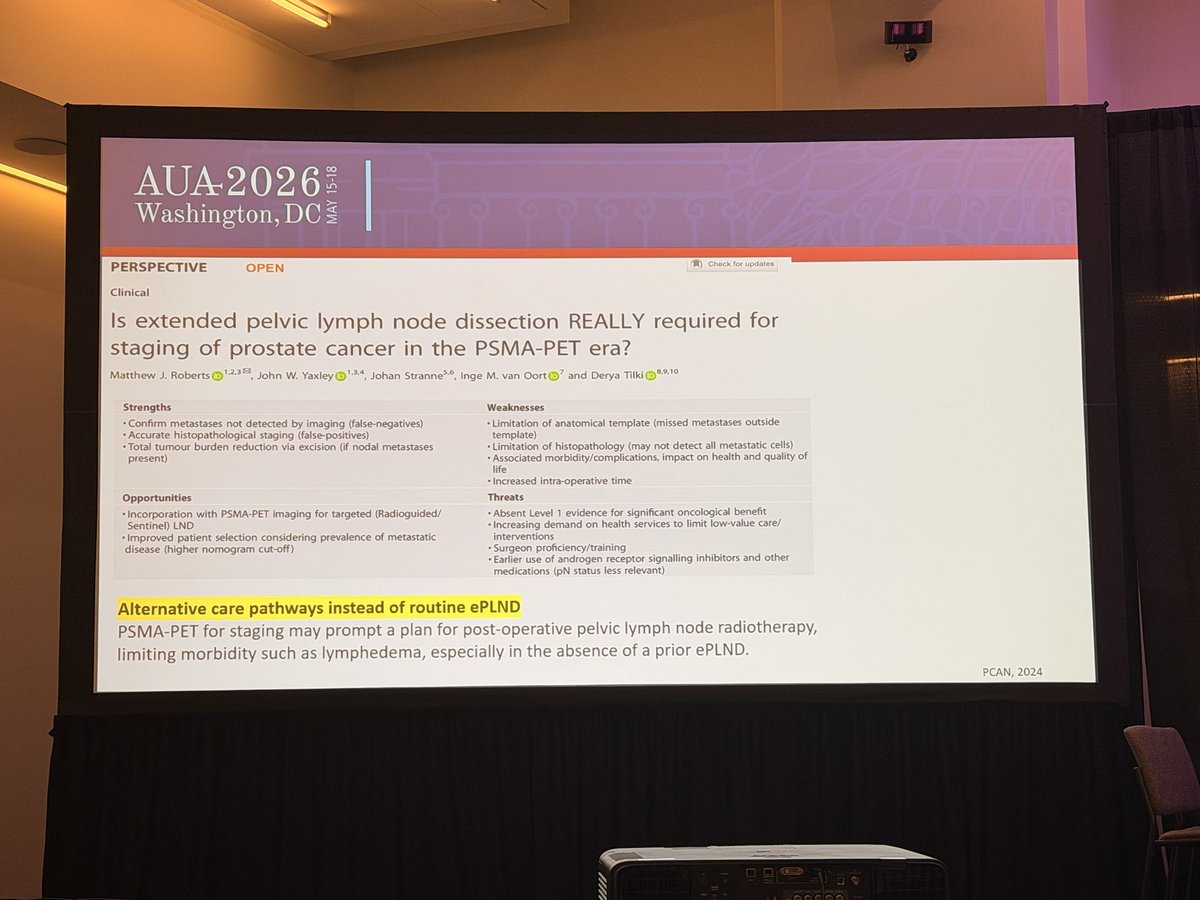
At #AUA2026, the message was clear: 📌 ePLND provides staging information, but its therapeutic benefit remains uncertain. 📌 RCTs have not shown consistent improvements in BCR outcomes. 📌 PSMA PET/CT has a high NPV (~96%) and may safely avoid unnecessary PLND in intermediate-risk patients with negative scans. 📌 Morbidity is not negligible: lymphedema, DVT/PE, and potential overtreatment. 📌 Up to 47% of nodal metastases may even lie outside the standard ePLND template.
The question is no longer “PLND yes or no?” 👉 It’s about smarter selection using PSMA PET, nomograms, and individualized risk assessment.
#ProstateCancer #PSMAPET
Comparison of #EMBARK and EAU criteria to identify high-risk patients with biochemical recurrence after radical prostatectomy. Presentation by Nadine Friedrich, MD @CedarsSinai. #AUA26 written coverage by @chavarriagaj > https://t.co/yyHo8ko8vo @AmerUrological
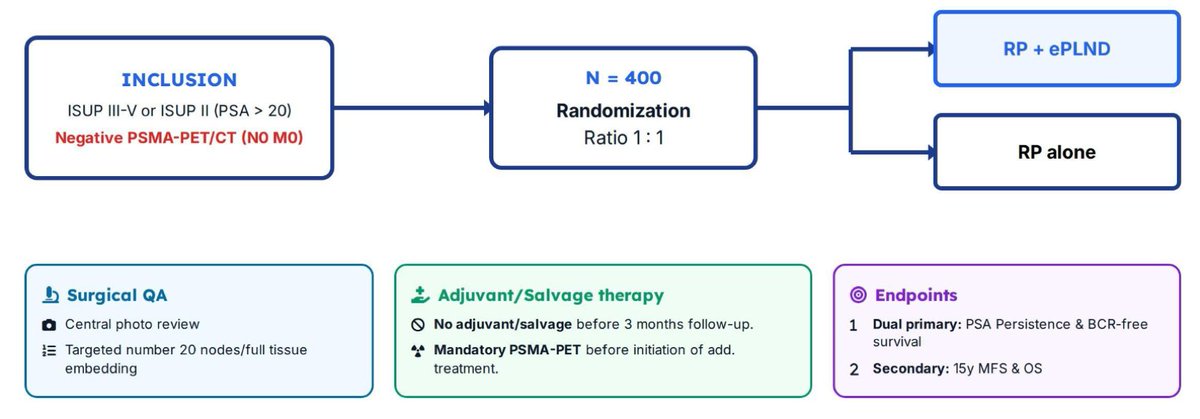
Does ePLND improve outcomes at RP in PSMA PET -ve HR PCa? @urotoday
Randomized DISSECTION 2.0 Ph 3 trial (#EAU26): RP + ePLND vs RP alone (n=400, 15 🇨🇭 centers)
Prim EPs:
• PSA persistence ≥0.1 ng/mL @ 3 mos
• BCR-FS
Results expected 2027
New in our partnership with @DGlaucomflecken: the KEYNOTE-905 trial evaluated enfortumab vedotin plus pembrolizumab as perioperative therapy in patients with muscle-invasive bladder cancer who were ineligible to receive cisplatin. Read the full study for free: https://t.co/A1RikB7ZIo
As the Clinical Lead at J&J at that time writing the #PROTEUS protocol and defining the specific PET-based MFS endpoint, I am curious to see the final official results at ASCO as well.
A few considerations:
🔵 As #PSMA PET imaging was not integrated in the study from the beginning, this endpoint will only be available for a subset of patients
🔵 PET based #MFS is defined in a specific way for PROTEUS as aligned with the FDA - not every positive PET scan counted
🔵 Subsequent therapy is important to consider which is often initiated prior to reaching conventional MFS
🔵 QoL is one key aspect to consider. Concerning erectile function, I’d expect that in cases with nerve sparing surgery and perioperative function (limited subset in a HR setting) recovery will be good
➡️ We will need to consider PROTEUS results together with results from other trials in this early setting including the #BCR setting
➡️ Finally, it will be most important to develop treatment strategies for patients resulting in as much as possible Freedom From Clinical Deterioration (FFCD) with as limited as possible subsequent treatment needed - new endpoints are needed! @ChrisSweens1@oncodaily@AttardLab@DrPaulNguyen #RadicalProstatectomy #ProstateCancer @TylerSbrt
A busy April wraps up with an outstanding prospective multi-institutional study on AS for small renal masses:
🔹Median FU 88 mo
🔹8-yr OS 88%
🔹Treatment-free survival 83%
🔹Only 17% required intervention
Tumour doubling time & location guide deferred active treatment plan.