How many out pts have No smoking , 0 risk factors are we watching fight aggressive bladder & kidney cancer with no answers? Too many. And the rates in are rising ⬆️
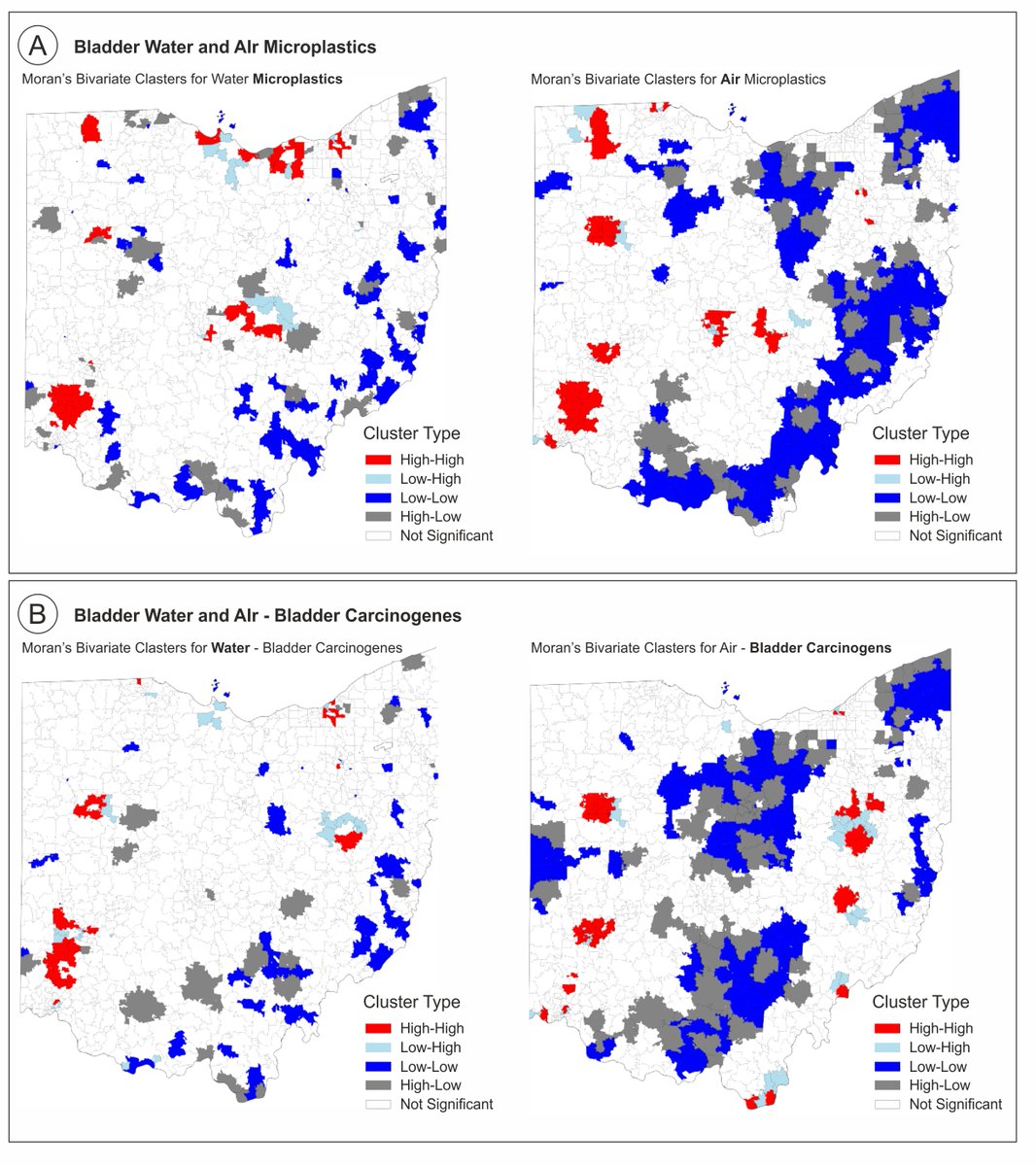
📝Our geospatial study found plastics processing 🫁air emissions correlate with bladder cancer incidence as strongly as known carcinogens
🌊Waterborne plastics tied to kidney cancer This is for our patients. Replicate it. Build on it. #BladderCancer #EnvironmentalHealth @CleClinicUro@UroOnc@UrolOncol
https://t.co/bbZzQYhA1Z. .
Proud of this one.☝️ The largest external validation of the @IBCG_BladderCA IR NMIBC model (n=2822) @CleClinicUro IR high ‼️11× the recurrence and 3yr progression 7%. Again showing heterogeneity within this group and individualized pt approach is needed .. using IBCG model will help inform their tx plan @EurUrolOncol
⚡️ First clinical validation of the EAU definitions of BCG failure in NMIBC (n=776).
BCG-refractory disease showed the highest progression rates: 46% at 5 years for HG recurrence at 6 months during maintenance. Early BCG-unresponsive recurrences conveyed similar progression risk to BCG-refractory disease (35% at 5 yr), supporting their inclusion in this category.
Prognostically informative definitions that can support clinical decision-making.
https://t.co/WPCzhGziY3
#BladderCancer #Oncology
🩺Outcomes of Intermediate Risk Non–muscle-invasive Bladder Cancer Receiving Adjuvant Treatment: A Pooled Analysis of Four Randomized Controlled Trials
by Wei Shen Tan...John D. Kelly et al
https://t.co/HfkqqTqneq
📢What does this study add?
This study presents a pooled analysis of individual patient data from four randomized controlled trials involving intermediate-risk (IR) non–muscle-invasive bladder cancer (NMIBC). The findings provide valuable estimates of recurrence and progression rates, which can inform clinical trial design, support accurate sample size calculations, and help optimize surveillance strategies for patients with IR-NMIBC.
🙌We thank the authors for trusting EUO with your work!
@drtanws@UroDocAsh@NPortaStat@AlbertoMartini@ahmostafid@EmmaHall71@Heer_Lab@uroweb@mroupret@GPloussard@jteoh_hk@Ric_Campi@CaPsurvivorship@LauraMarandino@RenuEapen@Ecastromarcos@OncoAlert@Sciencedirect
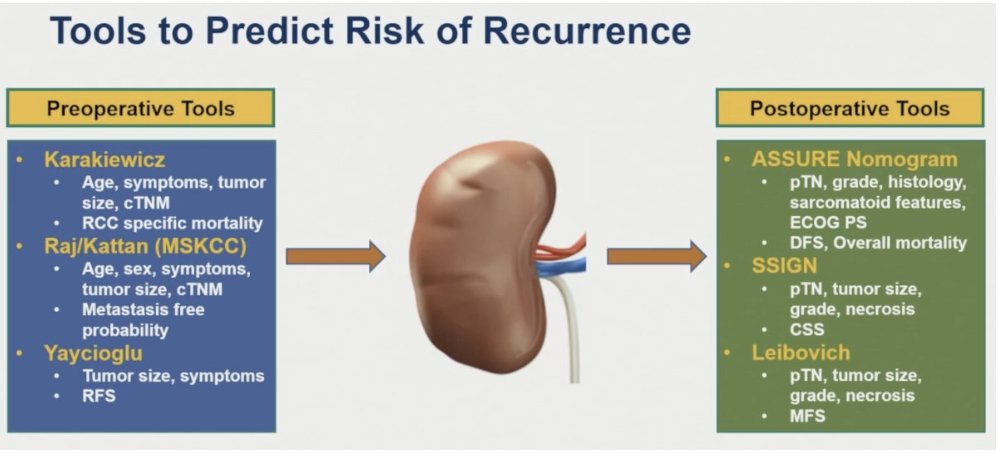
Glad our @EUplatinum RCC review is being utilized for AUA course review by an amazing teacher @drphil_urology 🙏 https://t.co/U4FdP8E6NH. Here is a nice overview of increasing incidence due to imaging 📈 with no change in mortality
New paper just out in @EurUrolOncol - outcomes of patients with intermediate-risk NMIBC when treated with contemporary protocols?
We analyzed 578 patients across 4 RCTs. IR NMIBC defined as per @IBCG_BladderCA and 2019 EAU Guidelines - only LG tumors.
Real-world relevant data. Here is what we found. 🧵
Ohttps://euoncology.europeanurology.com/article/S2588-9311%2826%2900127-6/fulltext
Today an other important opportunity to talk in the most important TVNEWS in Italy TG5 about one of the hot topic in #urology: #ERBC laser EN BLOC RESECTION OF BLADDER CANCER. Quick, easy, safer, better specimen for the pathologist to get a more reliable tumor staging. It should be offered whenever possible #ETCE
Magnitude and timing of clinical benefit associated with pathological complete response in perioperative #MIBC: A reconstructed IPD analysis of #NIAGARA trial. Presentation by Andrea Malgeri, MD @CampusBioMedico. #ASCO26 written coverage by @RKSayyid > https://t.co/hC9oyXrezJ @ASCO
🌄 Monday Morning Mention!
https://t.co/2tXgH9bFTu
🩺 AI-MIRACLE: Artificial Intelligence and MultIpaRAmetric MRI Predict CLinical OutcomEs to Neoadjuvant Immunotherapy in Patients with Muscle-invasive Bladder Cancer Undergoing Radical Cystectomy by Andrea Necchi...Lawrence H. Schwartz et al
💡 What does the study add?
The AI‑MIRACLE study highlights the necessity of rigorous model selection and demonstrates the substantial predictive value of post‑ immune-checkpoint inhibitors (ICI) multiparametric magnetic resonance imaging in muscle‑invasive bladder cancer. For pathological major response, the top‑performing models incorporated either post‑ICI radiomics alone or radiomics combined with dynamic contrast-enhanced features, whereas the optimal model for pathological complete response relied solely on post‑ICI radiomics. Across both endpoints, models integrating imaging features consistently outperformed benchmark models based only on clinical variables such as clinical stage, tumor mutational burden, and programmed cell-death-ligand-1 expression. These findings underscore the unique and clinically meaningful information provided by imaging‑derived biomarkers and support their potential role in response‑adaptive treatment strategies after neoadjuvant immunotherapy.
✨ We thank the authors trusting EUO to publish your work.
@uroweb@mroupret@GPloussard@jteoh_hk@Ric_Campi@CaPsurvivorship@LauraMarandino@RenuEapen@Ecastromarcos@OncoAlert@Sciencedirect
#ASCO26 GU highlight 🚨
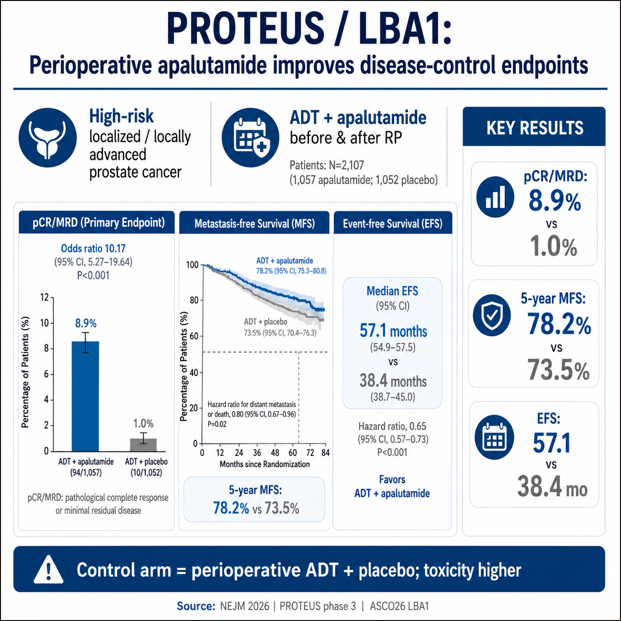
LBA1 PROTEUS
Perioperative apalutamide + ADT in high-risk localized / locally advanced prostate cancer
@ASCO@OncoAlert@NEJM
Presented by @MaryEllenTaplin
Published in @NEJM
https://t.co/0JWZmhn0df
This is a major perioperative prostate cancer dataset.
#PROTEUS tested 6 cycles of neoadjuvant + 6 cycles of adjuvant apalutamide added to ADT around radical prostatectomy.
Key results:
• pCR / minimal residual disease: 8.9% vs 1.0%
• 5-year metastasis-free survival: 78.2% vs 73.5%
• HR for distant metastasis or death: 0.80
• Event-free survival: 57.1 vs 38.4 months
• Time to first subsequent therapy: 74.2 vs 41.5 months
Why it matters:
For years, systemic perioperative intensification around prostatectomy has been difficult to establish in high-risk localized prostate cancer.
PROTEUS gives phase 3 evidence that deeper androgen-receptor pathway inhibition can improve pathologic response and delay clinically relevant recurrence events.
Important caveats:
This was not surgery alone vs systemic therapy.
The control arm received perioperative ADT + placebo.
MFS by conventional imaging alone was not significantly different.
Grade 3/4 AEs were higher with apalutamide, largely driven by rash.
My take:
This is practice-informing and potentially paradigm-shaping, but implementation will require careful patient selection, toxicity counseling, imaging context, and multidisciplinary discussion.
@EAntonarakis@DanaFarber_GU@DrChoueiri@montypal@tompowles1@brian_rini@PGrivasMDPhD@DrRanaMcKay@AliciaMorgans@amerseburger @NealShoreMD @DrYukselUrun@BraunMDPhD@DrSpratticus@EAntonarakis@KOSJ12@LoebStacy@apolo_andrea@AndreaNecchi@DrDanielHeng@neerajaiims@OncLive@TargetedOnc@CancerNetwrk@ASCOPost@VJOncology@ecancer
#ProstateCancer #GUonc #Oncology
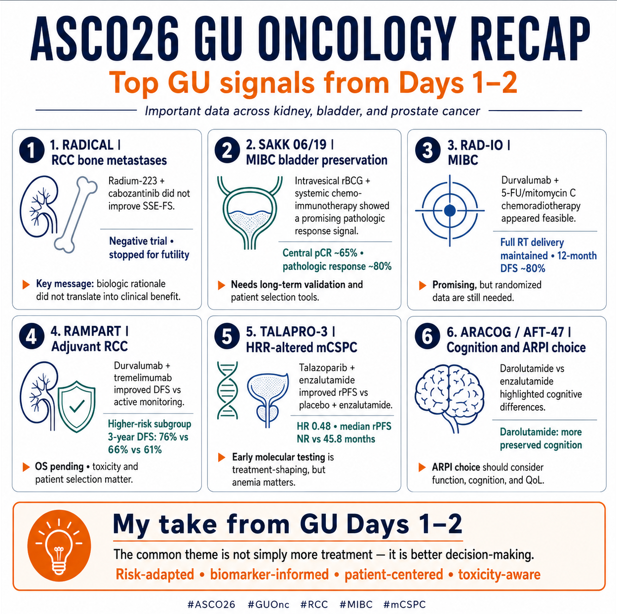
#ASCO26 GU Oncology Recap 🚨
🔬 Top GU signals from Days 1–2
Important data across kidney, bladder, and prostate cancer — not all practice-changing, but several clearly practice-informing.
Here are 6 GU signals I’m watching closely:
@OncoAlert@ASCO
🟧 1. #RADICAL#RCC bone metastases
Presented by @DrRanaMcKay
With GU colleagues/authors: @JoshLangMD@MattGalsky@TiansterZhang@DrChoueiri
Adding radium-223 to cabozantinib in RCC with bone metastases did not improve skeletal event–free survival.
The trial crossed its futility boundary and was stopped early.
Key message:
Bone metastases remain a major unmet need in RCC, but this biologically attractive strategy did not translate into clinical benefit.
Negative trials matter when they close doors clearly.
🟦 2. #SAKK 06/19 #MIBC bladder preservation
Presented by Richard Cathomas
With GU collaborators including @UrsulaVogl
A bladder-preserving strategy using intravesical rBCG + systemic chemo-immunotherapy showed a very promising pathologic response signal.
Reported central pCR was ~65%, with pathologic response ~80%.
Key message:
Bladder preservation is moving beyond classic trimodality therapy.
But we still need careful validation, long-term local control, cystectomy-free survival, and patient selection tools.
🟩 3. #RAD-IO #Durvalumab + chemoradiotherapy in MIBC
Presented by Nicholas D. James
Durvalumab with 5-FU/mitomycin C chemoradiotherapy appeared feasible.
Important delivery signal:
• full RT delivery was maintained
• chemotherapy delivery was largely preserved
• 12-month DFS was encouraging, around 80%
Key message:
Adding IO to bladder-directed CRT is promising, but follow-up is short and randomized data are still needed before changing routine bladder-preservation algorithms.
🟨 4. #RAMPART |Adjuvant RCC
Presented by James Larkin
With key RCC colleagues including @DrChoueiri@tompowles1
Durvalumab + tremelimumab improved DFS vs active monitoring after resection of RCC, with the clearest signal in higher-risk disease.
Higher-risk subgroup:
• 3-year DFS: 76% with durva+trem
• 66% with durva alone
• 61% with active monitoring
Key message:
Adjuvant RCC is becoming more nuanced.
The signal is important, but OS is pending, toxicity matters, and patient selection remains central.
This should not become a “treat everyone” message.
🟥 5. #TALAPRO-3 HRR-altered mCSPC
Presented by @neerajaiims
Talazoparib + enzalutamide significantly improved investigator-assessed rPFS vs placebo + enzalutamide in HRR-altered metastatic castration-sensitive prostate cancer.
Key result:
• HR 0.48
• median rPFS not reached vs 45.8 months
• benefit seen in BRCA and non-BRCA HRR subgroups
But toxicity matters:
Anemia was the major safety signal.
Key message:
Early molecular testing is becoming treatment-shaping in prostate cancer.
But PARP + ARPI intensification should remain biologically selected and toxicity-aware.
🟪 6. #ARACOG / AFT-47 Cognition and ARPI choice
Presented by @AliciaMorgans
Darolutamide vs enzalutamide was studied with cognitive endpoints using CANTAB testing.
Key clinical signal:
• darolutamide-treated patients showed patterns consistent with preserved learning effect/stable cognition
• enzalutamide-treated patients had more stable-to-decreased cognitive scores
• crossover was striking: 30 from enzalutamide to darolutamide vs 0 in the reverse direction
Key message:
ARPI choice is not only about tumor control.
For many patients, cognition, falls, neurologic toxicity, function, and quality of life are part of the treatment decision.
💬 My take from GU Days 1–2
The common theme is not simply “more treatment.”
It is better decision-making:
✓ who needs intensification?
✓ who can avoid unnecessary toxicity?
✓ which biomarkers are actionable?
✓ how do we preserve bladder, cognition, function, and quality of life?
✓ how do we interpret promising early signals without overextending them?
The future of GU oncology is increasingly:
risk-adapted, biomarker-informed, patient-centered, and toxicity-aware.
#ASCO26 #GUOnc #KidneyCancer #BladderCancer #ProstateCancer #RCC #MIBC #mCSPC #PrecisionOncology #Immunotherapy #PARPInhibitors #PatientCenteredCare
@DrChoueiri 🇺🇸 @hoperugo 🇺🇸 @matteolambe 🇮🇹 @TiansterZhang 🇺🇸 @CathyEngMD 🇺🇸 @stolaney1 🇺🇸 @montypal 🇺🇸 @tompowles1 🇬🇧 @brian_rini 🇺🇸 @cdanicas 🇪🇸 @NiuSanford 🇺🇸 @amerseburger 🇩🇪 @GlopesMd 🇺🇸 @Icro_Meattini 🇮🇹 @PGrivasMDPhD 🇺🇸 @DrYukselUrun 🇹🇷 @nataliagandur 🇦🇷 @ElisaAgostinett 🇧🇪 @HHorinouchi 🇯🇵 @realbowtiedoc 🇺🇸 @to_be_elizabeth 🇮🇹 @UOzkerim 🇹🇷 @p_ciracimd 🇮🇹 @DrVilmaPBarcia 🇪🇸 @DraMartinezLago 🇪🇸 @DrMirallas 🇺🇸 @GaiaGriguolo 🇮🇹 @MarioBalsaMD 🇪🇸 @scocmem 🇬🇧 @AmandaNizamMD 🇺🇸 @weoncologists 🇺🇸
#ASCO26 GU Oncology Spotlight 🚨
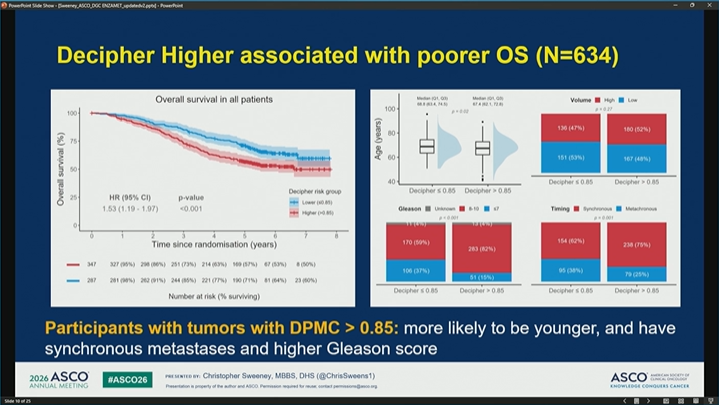
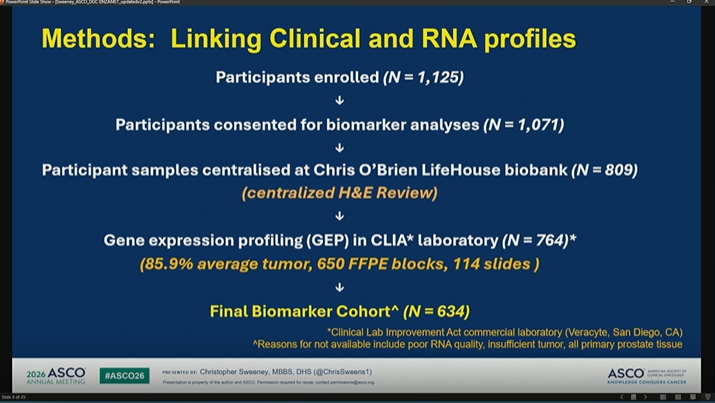
🔬 ENZAMET + Decipher Prostate Classifier
Genomics to refine docetaxel intensification in mHSPC
As always, an outstanding and very clear presentation by @ChrisSweeney1.
Thank you, Dr. Sweeney.
@OncoAlert@ASCO
In metastatic hormone-sensitive prostate cancer, treatment intensification has changed outcomes.
But one of the hardest clinical questions remains:
➡️ Who truly needs more intensification?
➡️ Who benefits from adding docetaxel to ADT + enzalutamide?
➡️ Can biology help us avoid both undertreatment and overtreatment?
🟦 Why ENZAMET matters here
ENZAMET was an investigator-sponsored study evaluating:
• ADT + standard non-steroidal antiandrogen
vs
• ADT + enzalutamide
Importantly, the study later allowed planned early docetaxel after CHAARTED, creating a unique opportunity to explore:
🧬 ADT + enzalutamide ± docetaxel
This is highly relevant to modern mHSPC decision-making.
🟩 Why Decipher is important
The Decipher Prostate Genomic Classifier uses a 22-gene mRNA signature.
It is designed to capture biologic features linked to:
🔹 metastatic potential
🔹 prognosis
🔹 disease aggressiveness
🔹 pathways such as DNA replication/repair, cell motility, and growth biology
In this analysis, higher Decipher scores were associated with poorer overall survival.
🟨 The key hypothesis
Patients with tumors showing Decipher >0.85 may represent a biologically higher-risk group.
The study asked:
➡️ Could this group derive greater survival benefit from adding docetaxel to ADT + enzalutamide?
And conversely:
➡️ Could patients with Decipher ≤0.85 avoid docetaxel without losing meaningful benefit?
🟧 Why this question matters clinically
Docetaxel can be effective.
But it also adds:
• toxicity
• clinic visits
• supportive care needs
• neuropathy risk
• infection risk
• quality-of-life impact
• access and feasibility issues
So the goal is not simply to add docetaxel to everyone.
The goal is to use clinical + genomic risk to better personalize treatment.
🟥 Take-home from Part 1
This is exactly where prostate cancer care is heading:
Not only asking:
“Can we intensify?”
But asking:
“Who needs intensification most — and who can safely avoid it?”
Part 2: results + clinical interpretation 👇
@DrChoueiri 🇺🇸@hoperugo 🇺🇸 @matteolambe 🇮🇹 @TiansterZhang 🇺🇸 @CathyEngMD 🇺🇸 @stolaney1 🇺🇸 @montypal 🇺🇸 @tompowles1 🇬🇧 @brian_rini 🇺🇸 @cdanicas 🇪🇸 @NiuSanford 🇺🇸 @amerseburger 🇩🇪 @GlopesMd 🇺🇸 @Icro_Meattini 🇮🇹 @PGrivasMDPhD 🇺🇸 @DrYukselUrun 🇹🇷
#ASCO26 #GUOnc #ProstateCancer #mHSPC #PrecisionOncology #Genomics #Decipher #Docetaxel #Enzalutamide
#ASCO26 GU Oncology Spotlight 🚨
🔬 Management in Bladder Cancer After Pathologic Complete Disease Response
Presented by Brendan J. Guercio, MD
@OncoAlert@ASCO
In muscle-invasive bladder cancer, pCR after neoadjuvant therapy is one of the most powerful prognostic signals we have.
But the key clinical question is becoming more complex:
➡️ If a patient achieves pCR after perioperative therapy, should we continue adjuvant treatment — or stop?
Historically, pCR after neoadjuvant chemotherapy has been associated with excellent outcomes.
In SWOG 8710:
• pT0 after neoadjuvant chemotherapy → ~85% 5-year OS
Meta-analyses also support pCR as a strong positive prognostic marker for recurrence-free survival.
So pCR matters.
But pCR is not the same as proof that postoperative therapy is unnecessary.
📌 Current MIBC perioperative landscape is changing fast
For cisplatin-ineligible or cisplatin-declining patients:
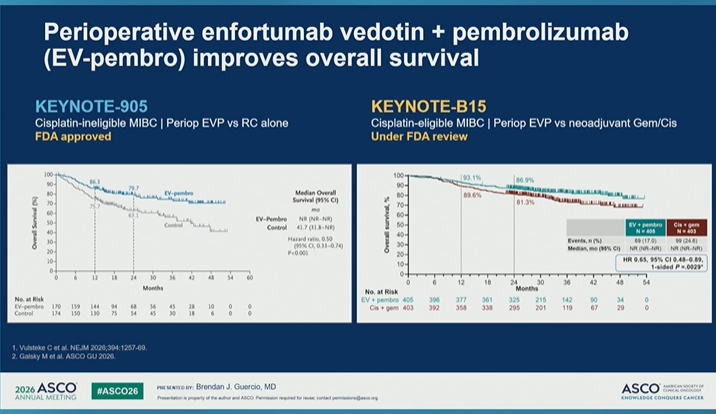
• KEYNOTE-905 / EV-303: perioperative EV + pembrolizumab is now a major standard-setting approach
• VOLGA: perioperative EV + durvalumab ± tremelimumab adds another immune/ADC-based strategy
For cisplatin-eligible patients:
• NIAGARA: Gem/Cis + perioperative durvalumab improved outcomes
• VESPER: ddMVAC improved survival vs Gem/Cis but with greater toxicity
• KEYNOTE-B15: perioperative EV + pembrolizumab improved OS vs Gem/Cis-based treatment
The field is clearly moving toward immunotherapy-based “sandwich” regimens.
🧭 Management after pCR: continue or stop?
Current standard practice remains:
➡️ Continue planned adjuvant therapy for perioperative sandwich regimens, regardless of pathologic response.
Examples:
• NIAGARA: resume durvalumab post-cystectomy
• Perioperative EV + pembrolizumab: resume planned postoperative therapy
• Cisplatin-based chemo alone with pCR: surveillance remains standard
Why?
Because we still do not know the relative contribution of:
🔹 the neoadjuvant component
🔹 the postoperative/adjuvant component
🔹 surgery
🔹 pathologic response itself
🔹 underlying tumor biology
⚠️ Unanswered question
Can adjuvant therapy be safely de-escalated based on pCR?
Not yet.
pCR is prognostic.
But we still need prospective evidence to determine whether it is predictive enough to guide treatment discontinuation.
This is especially important because postoperative therapy may add:
• toxicity
• neuropathy
• immune-related adverse events
• treatment burden
• cost
• delays in recovery
• impact on quality of life
💬 My take
pCR is an excellent sign — but it is not yet a permission slip to stop planned adjuvant therapy after modern perioperative regimens.
For now, the safest message is:
➡️ follow the regimen as tested
➡️ discuss toxicity and recovery
➡️ avoid unproven de-escalation outside trials
➡️ develop biomarkers that can identify who truly needs postoperative treatment
The next frontier in MIBC is not only achieving pCR.
It is learning how to use pCR — together with biomarkers and patient outcomes — to personalize escalation and de-escalation.
@DrChoueiri 🇺🇸@hoperugo 🇺🇸 @matteolambe 🇮🇹 @TiansterZhang 🇺🇸 @CathyEngMD 🇺🇸 @stolaney1 🇺🇸 @montypal 🇺🇸 @tompowles1 🇬🇧 @brian_rini 🇺🇸 @cdanicas 🇪🇸 @NiuSanford 🇺🇸 @amerseburger 🇩🇪 @GlopesMd 🇺🇸 @Icro_Meattini 🇮🇹 @PGrivasMDPhD 🇺🇸 @DrYukselUrun 🇹🇷
@ecancer@urologysummit@UrologyTimes
#ASCO26 #GUOnc #BladderCancer #UrothelialCancer #MIBC #pCR #EVPembro #Immunotherapy #PrecisionOncology
Lets think about this.. Biologically 🧬 speaking this makes 0 sense
🇧🇷BCG is not tumor ablative ( this has been tried and failed miserably), 3 treatments (78% of pt) & we know maintenance is critical
⚽️pCR 68% is huge leap from previous GC+atezo alone(pCR 41% w/o rBCG (without n1)...
and lets not forget 11% of this cohort was N1 and majority not fully resected. The results are provocative but I would love to see this replicated ( I am keeping an open mind)
some reads >> pCR 41% with GC atezo https://t.co/AmEBOIO0GU
BCG in mibc> https://t.co/vtBGJs9PuY