Happy Father’s Day to the fathers of oncology.
Sidney Farber taught us cancer could be treated.
Paul Ehrlich taught us cancer could be targeted.
James Allison taught us the immune system could fight back.
Every modern oncology clinic stands on the shoulders of giants.
#FathersDay #Oncology #CancerResearch #MedTwitter
@OncoAlert@Larvol@DanaFarber
🔬 TESTICULAR GERM CELL TUMORS: KNOW YOUR TUMOR MARKERS
Serum tumor markers are more than just numbers—they guide diagnosis, staging, prognosis, treatment response, and relapse detection in testicular germ cell tumors (GCTs).
📌 AFP
✔ Elevated in yolk sac tumors, embryonal carcinoma, and mixed GCTs
✔ NEVER elevated in pure seminoma
📌 β-hCG
✔ Highest in choriocarcinoma
✔ May be mildly elevated in seminoma
✔ Can cause gynecomastia and hyperthyroidism when markedly elevated
📌 LDH
✔ Reflects tumor burden
✔ Important prognostic marker in IGCCCG risk classification
🚨 High-Yield Pearl:
Persistent elevation of tumor markers after orchiectomy suggests residual disease (Stage IS).
🧬 Future of GCT Biomarkers:
miR-371a-3p is emerging as a highly sensitive and specific marker for active germ cell tumors and may transform surveillance strategies in the coming years.
Early detection. Accurate staging. Better outcomes.
#TesticularCancer #GermCellTumor #MedicalOncology #Oncology #UroOncology #Seminoma #NSGCT #AFP #BetaHCG #LDH #CancerEducation #MedEd #FOAMed #OncologyTeaching #MedicalStudents #Residents #DrRupamManna #CancerConceptsExplained
OPTIMA Trial #ASCO2026
One of the most important lessons from ASCO 2026:
Clinical high risk ≠ Genomic high risk.
Among patients with clinically high-risk ER+/HER2− early breast cancer, 68% had low genomic risk (ROR ≤60).
A PAM50-guided treatment strategy substantially reduced chemotherapy use while preserving outcomes:
📊 5-year IBCFS: 90.4% vs 91.5%
📊 HR 0.99 (Non-inferior)
Key takeaway:
🧬 Biology and clinical risk are not the same.
💉 Less chemotherapy is possible for many patients.
✅ Outcomes remained preserved.
Stein et al. #ASCO2026
#BreastCancer #Oncology #PrecisionOncology #MedTwitter #MVOnco
Presented at #ASCO26:
In patients with metastatic prostate cancer with gene alterations, talazoparib–enzalutamide led to better progression-free survival outcomes than placebo–enzalutamide but with more serious adverse events. Full phase 3 TALAPRO-3 trial results: https://t.co/MFVGDGwPzc
Editorial: Precision Intensification in Metastatic Prostate Cancer https://t.co/Q7rjJJ7wJL
@ASCO
#ASCO26 through an algorithm lens
@ASCO@tompowles1
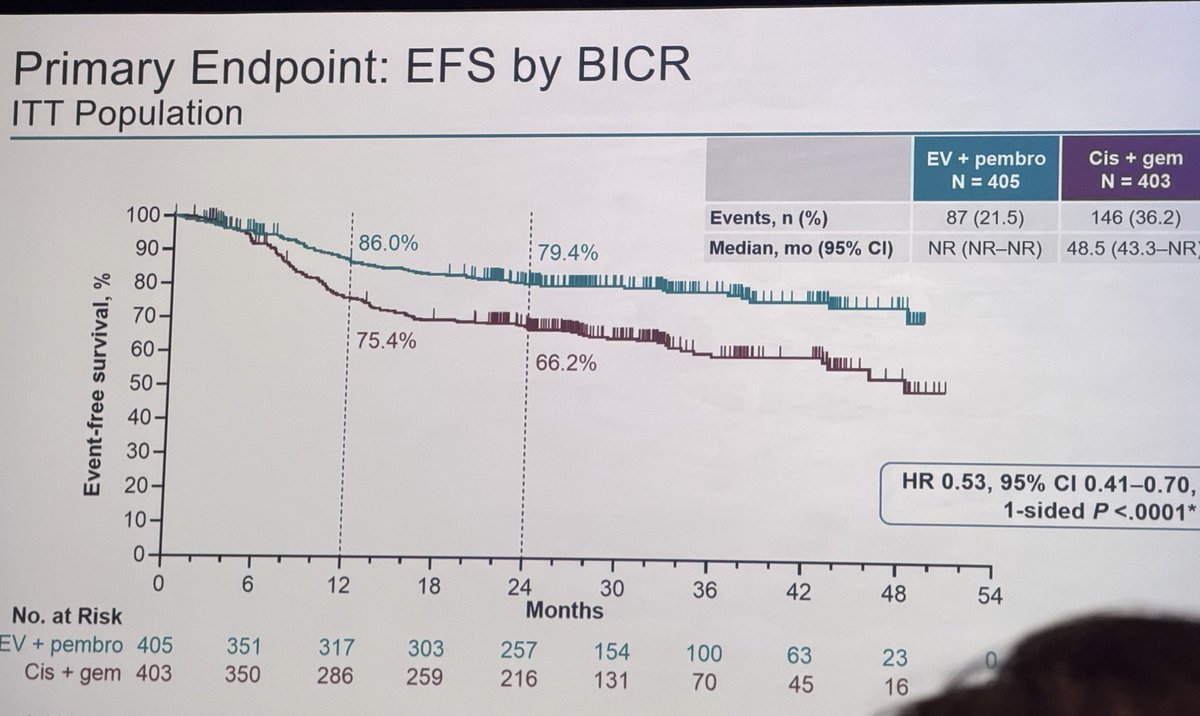
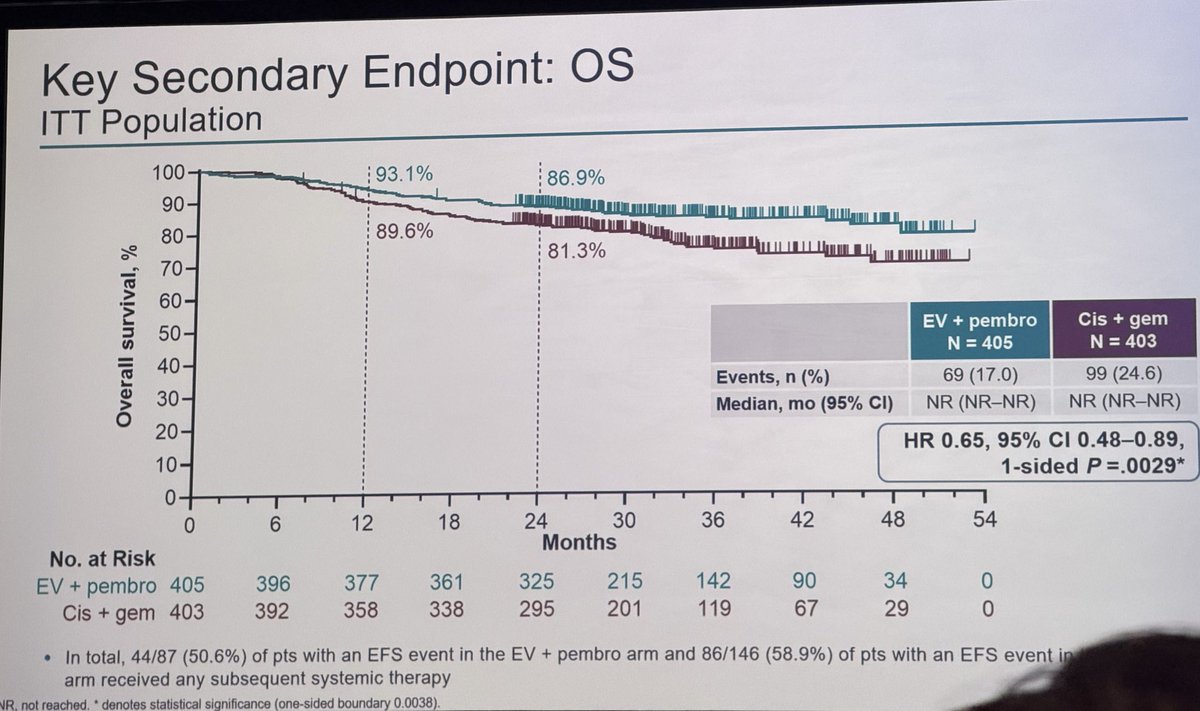
Study: EV-302 / KEYNOTE-A39
Abstract 4507 | 1L locally advanced/metastatic urothelial carcinoma
Clinical decision point:
What should be the preferred first-line systemic therapy for eligible patients with la/mUC?
Potential algorithm impact:
This update strengthens the current 1L EV+pembrolizumab pathway. With durable OS benefit at 3.5 years and no new safety signal, the algorithmic question shifts from “is this preferred?” to “who is eligible, how do we monitor toxicity, and what comes next?”
What is strengthened:
EV+P remains a high-confidence 1L option when accessible and clinically appropriate.
What remains uncertain:
Post-EV+P sequencing, treatment duration, management in frail patients, and implementation in settings where EV access is limited.
Bottom line:
The first-line mUC algorithm is increasingly shaped by EV+P — but implementation requires toxicity infrastructure, cost/access planning, and a sequencing strategy.
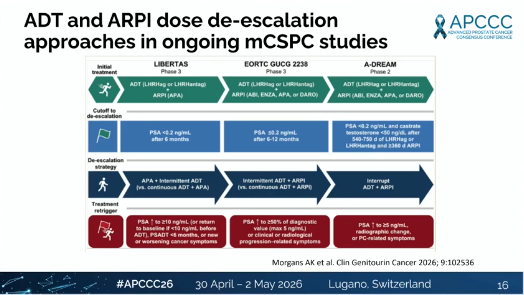
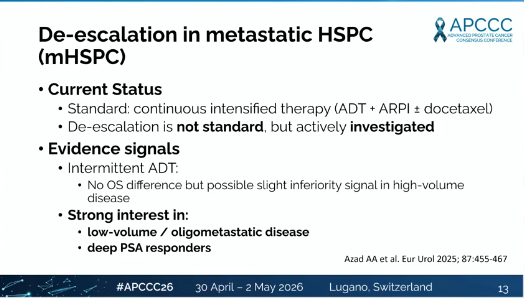
⭐ De-escalation in mHSPC can we safely treat less?
@OncoAlert@APCCC_Lugano#APCCC26@Silke_Gillessen@AOmlin
Presented by Mika P. Matikainen
👏 Excellent, forward-looking presentation
🔹 Thought-provoking and clinically important talk
🔹 Key insights:
🔵 EMBARK introduces a modern de-escalation model
• PSA-guided treatment suspension
• A significant proportion remain off therapy >2 years
🔵 Current standard → continuous intensification
• De-escalation not yet standard, but rapidly evolving
🔵 Who may benefit?
• Low-volume / oligometastatic disease
• Deep PSA responders
• Favorable biology
🔵 Intermittent strategies:
• Similar OS in selected patients
• Possible trade-offs in high-volume disease
🔵 Future direction:
• Shift from empirical → biomarker-driven de-escalation
• Ongoing trials testing adaptive, response-guided strategies
🔹 Key unanswered questions:
• Optimal PSA thresholds to stop/restart
• Role of PSMA-defined disease burden
• Can ARPI monotherapy replace long-term ADT?
🔹 Take-home:
De-escalation is no longer hypothetical →
but precision selection is critical before changing practic
@ecancer@urologysummit @MedicalwatchHQ @urotoday
#ProstateCancer #UroOncology #Oncology
⭐ Molecular sub-grouping of mHSPC — who benefits from what? (PART 2)
@OncoAlert@APCCC_Lugano#IPCS26#APCCC26@Silke_Gillessen@AOmlin
Presented by G. Attard
🔹 Key messages:
🔹 1. Alterations in HRR genes (especially BRCA1/2) are associated with worse overall survival
🔹 2. HRR status is not only prognostic → it is predictive for PARP inhibitor benefit
🔹 3. In AMPLITUDE, niraparib + AAP significantly improved rPFS in HRR-mutated patients
🔹 4. Genomic testing (BRCA/HRR) should be integrated early in mHSPC decision-making
🔹 5. Transcriptomic classifiers (e.g. PAM50) may help identify who benefits from docetaxel
🔹 6. Future treatment selection will rely on combined genomic + transcriptomic stratification
🔹 Take-home:
mHSPC management is shifting toward biology-driven treatment selection (ARPI vs chemo vs PARPi)
@Silke_Gillessen@JTheurillat@mishabeltran@bjartell@ChrisSweens1@DrMHofman@ProfKHerrmann@tompowles1@EAntonarakis@declangmurphy@VedangMurthy@KOSJ12@LoebStacy
1/
Obesity causes cancer. 🧵
Not "might." Not "is linked to."
10% of all new cancers in the US.
Up to 50% of endometrial and kidney cancers.
This is not a lifestyle conversation. It's oncology.
@JAMA_current
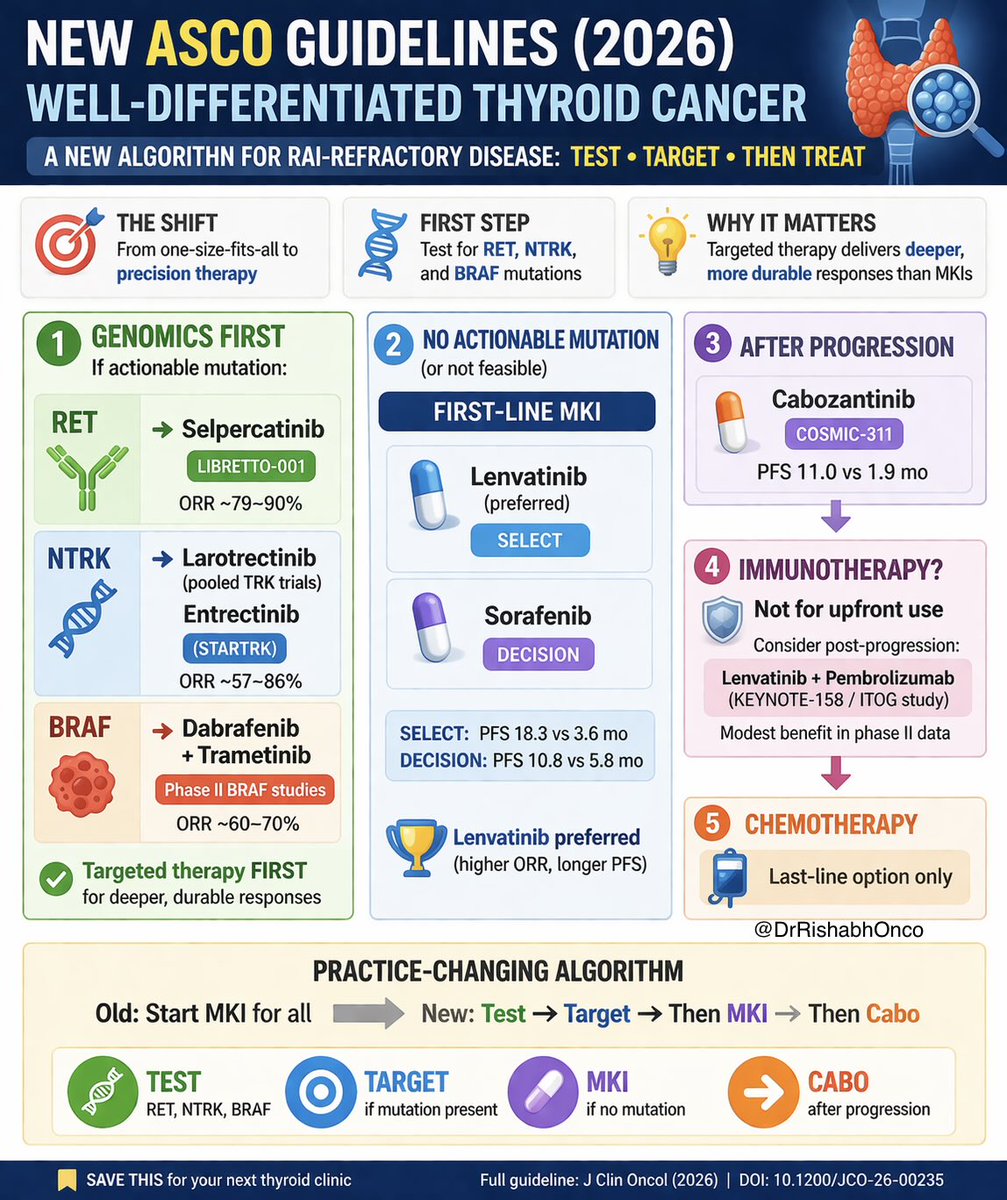
🚨 New ASCO Guidelines (2026): Well-Differentiated Thyroid Cancer
This is a major shift in how we treat RAI-refractory disease 👇
🧠 Step 1 is no longer MKI… it’s GENOMICS
👉 Test for: RET | NTRK | BRAF
If actionable → Targeted therapy FIRST
• RET → Selpercatinib (LIBRETTO-001)
• NTRK → Larotrectinib (pooled TRK trials) / Entrectinib (STARTRK)
• BRAF → Dabrafenib ± Trametinib (phase II BRAF studies)
🔥 Deep, durable responses > MKIs
📊 Signal strength
• NTRK inhibitors → ORR ~57–86%
• RET inhibitors → ORR ~79–90%
🧠 If no mutation (or not feasible)
👉 First-line MKI
• Lenvatinib (SELECT)
• Sorafenib (DECISION)
📊
SELECT → PFS 18.3 vs 3.6 mo
DECISION → PFS 10.8 vs 5.8 mo
👉 Lenvatinib preferred (higher ORR, longer PFS)
🧠 After progression
👉 Cabozantinib (COSMIC-311)
📊 PFS 11.0 vs 1.9 mo
🧠 Immunotherapy?
❌ Not upfront
👉 Consider only post-progression
Lenvatinib + Pembrolizumab (KEYNOTE-158 / ITOG study)
🧠 Chemotherapy
👉 Last-line only
🎯 Practice-changing shift
Old → Start MKI for all
New → Test → Target → Then MKI → Then Cabo
💡 Thyroid cancer is now a precision oncology disease
🔖 Save this before your next thyroid clinic
#OncoTwitter #MedTwitter #ThyroidCancer #PrecisionOncology @OncoAlert@myesmo@esmo_open@asco
‼️❓Is trusting only PSA reasonable in metastatic prostate cancer?
🚨Post hoc analysis of ARCHES + PROSPER shows PSA can miss radiographic progression on enzalutamide.
🚨Among patients with radiological progression, 25% had no PSA rise and 60% did not meet PSA progression criteria.
‼️‼️Imaging-only progression also predicted worse OS.
👉https://t.co/poHSHZG9Id
@JCO_ASCO@ASCO@OncoAlert@APCCC_Lugano@urotoday@DrYukselUrun
🧠 Thinking Like an Elite Oncologist – Daily Checklist
🔍 1. DIAGNOSIS: “Do I truly understand this tumor?”
Histology confirmed?
Stage accurate (any missed metastasis?)
Is this typical or atypical biology?
Could this be a different primary or mixed histology?
👉 Elite move: Always question the obvious.